

Quality Improvement Initiative Enhances Outpatient Pediatric Pulmonology Follow-up for Premature Infants with Bronchopulmonary Dysplasia
- PMID: 38854502
- PMCID: PMC11161285
- DOI: 10.1097/pq9.0000000000000736
Quality Improvement Initiative Enhances Outpatient Pediatric Pulmonology Follow-up for Premature Infants with Bronchopulmonary Dysplasia
Abstract
Introduction: Bronchopulmonary dysplasia (BPD) is a chronic lung disorder affecting many premature infants. Infants with BPD have higher hospital readmission rates due to respiratory-related morbidity. We aimed to increase the rates of outpatient pulmonary follow-up and attendance of premature babies with moderate and severe BPD to above 85% within 6 months.
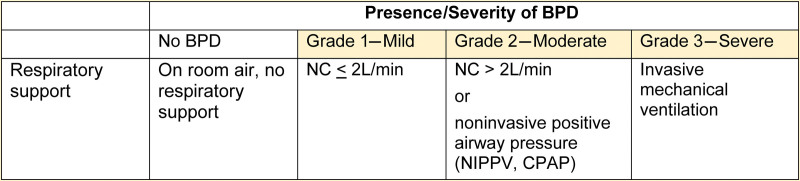
Methods: We conducted a quality improvement project at Yale New Haven Children's Hospital. Key interventions included developing a BPD clinical pathway integrated into the electronic medical record to assist providers in correctly classifying BPD severity, assigning the appropriate International Classification of Diseases, 10th Revision code (P27.1), and providing standardized treatment options. The outcome measures included correct diagnosis and classification of BPD, the percentage of patients with BPD scheduled for pediatric pulmonology appointments within 45 days, and the percentage attending those appointments.
Results: There were 226 patients in our study, including 85 in the baseline period. Correct diagnosis of BPD increased from 49% to 95%, the percentage of scheduled appointments increased from 71.9% to 100%, and the percentage of appointments attended increased from 55.6% to 87.1%.
Conclusions: Our quality improvement initiative improved the accuracy of diagnosis, severity classification, and outpatient pulmonary follow-up of children with moderate and severe BPD.
Copyright © 2024 the Author(s). Published by Wolters Kluwer Health, Inc.
Figures





References
-
- Shennan AT, Dunn MS, Ohlsson A, et al. . Abnormal pulmonary outcomes in premature infants: prediction from oxygen requirement in the neonatal period. Pediatrics. 1988;82:527–532. - PubMed
LinkOut - more resources
Full Text Sources