

Race, age at diagnosis and histological characteristics of lung cancer in never-smokers (LCINS) and ever-smokers in low-dose computed tomography (LDCT) screening: a systematic review and meta-analysis
- PMID: 38854936
- PMCID: PMC11157373
- DOI: 10.21037/tlcr-23-816
Race, age at diagnosis and histological characteristics of lung cancer in never-smokers (LCINS) and ever-smokers in low-dose computed tomography (LDCT) screening: a systematic review and meta-analysis
Abstract
Background: We previously demonstrated in a meta-analysis there was no difference in risk ratio (RR) of lung cancer detected by low-dose computed tomography (LDCT) screening among female never-smokers (NS) and male ever-smokers (ES) in Asia. LDCT screening significantly decreased lung cancer death among Asian NS compared to Asian ES (RR =0.27, P<0.001).
Methods: We investigated if race, age at diagnosis, and histology further differentiate lung cancer diagnosed by LDCT among in NS and ES using the 14 studies from our previous meta-analysis.
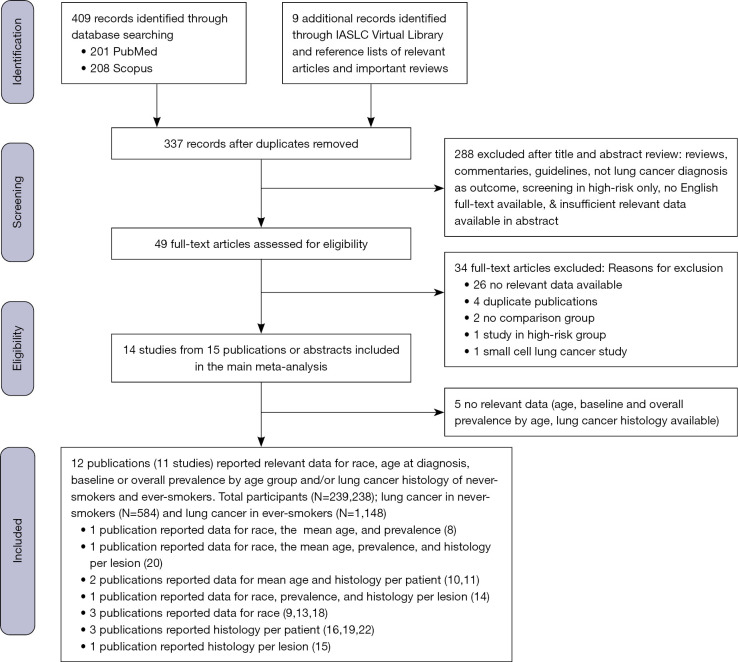
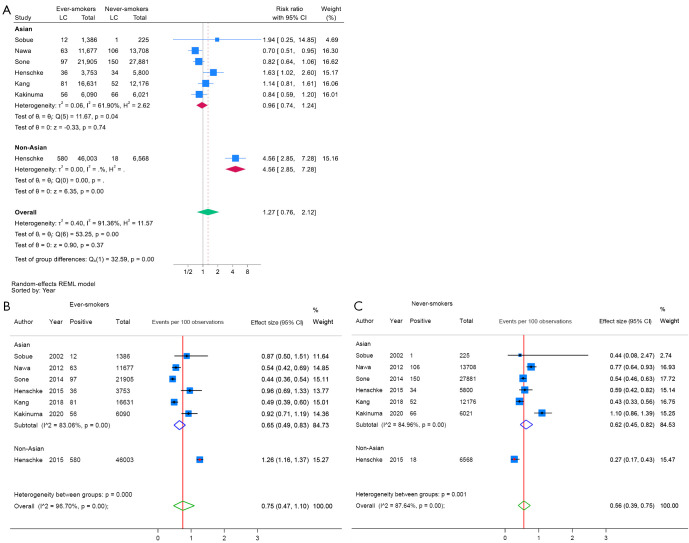
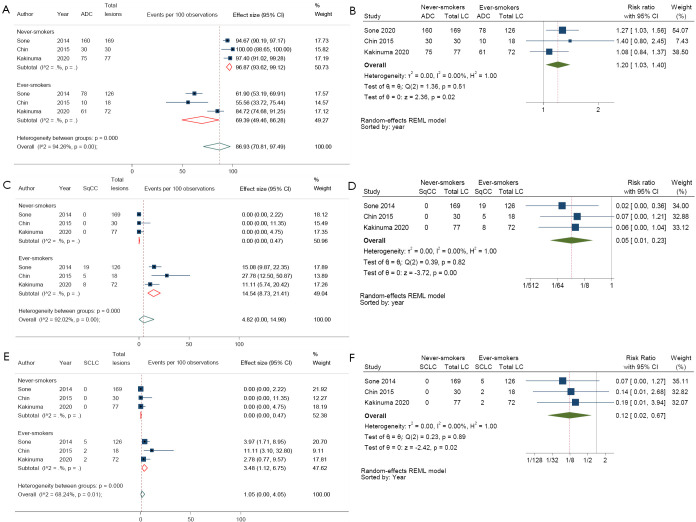
Results: Twelve publications reported relevant data utilized in this study. From five Asian and one international studies, Asian ES had similar risk of lung cancer diagnosed at baseline screening as Asian NS [RR =0.96; 95% confidence interval (CI): 0.74-1.24] but among non-Asian ES had a 4.56 times significantly higher risk than non-Asian NS (RR =4.56; 95% CI: 2.85-7.28). The baseline incidence of lung cancer in never-smoker (LCINS) was approximately 2.3 times higher among Asian NS than non-Asian NS (0.62% vs. 0.27%, P=0.001). Asian ES had about half the baseline incidence of lung cancer diagnosed as non-Asian ES (0.65% vs. 1.26%). LCINS was diagnosed at 1.98 years younger than ES (95% CI: -3.38 to -0.58) (four studies) and exhibited a higher proportion of adenocarcinoma (ADC) (96.58% vs. 70.37%).
Conclusions: Among normal-risk individuals, LCINS had a significantly higher likelihood of being diagnosed among Asians than non-Asians, predominantly manifesting as ADC and diagnosed approximately 2 years younger than ES suggesting that the age limit to initiate lung cancer screening in NS may be set lower compared to LDCT lung cancer screening among ES.
Keywords: Meta-analysis; low-dose computed tomography screening (LDCT screening); lung cancer in never-smokers (LCINS).
2024 Translational Lung Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tlcr.amegroups.com/article/view/10.21037/tlcr-23-816/coif). S.H.I.O. serves as an Associate Editor-in-Chief of Translational Lung Cancer Research from August 2023 to July 2025. N.T. got payment or honoraria for lectures or presentations from AstraZeneca, Roche, and Thoracic Society of Thailand under Royal Patronage (TST) in the past 36 months; got support for attending meetings from AstraZeneca, Roche, TST, IASLC, and I-ELCAP in the past 36 months. M.N. received consulting fees from Pfizer, Lilly, Novartis, Jassen, Daiichi Sankyo, BMS, AnHeart Therapeutics, J Inst Bio and BluePrint Medicines within the past 36 months; got payment or honoraria for lectures or presentations from Pfizer, Janssen, Dava Oncology LLP, EMD Sereno, OncLive, Takeda, Caris Life Science and Mirati within the past 36 months; got support for attending meetings from AnHeart Therapeutics within the past 36 months; and has stock ownership in MBrace Therapeutics within the past 36 months. E.S. received research grant from Delfi Diganostics within the last 36 months; received consulting fees from Astra Zeneca, Boerhinger Ingelheim, Janssen, and Genentech within the last 36 months; and received lecture fees from OncLive within the past 36 months. S.H.I.O. received consulting fees from Pfizer, Lilly, Jassen, Daiichi Sankyo, BMS, AnHeart Therapeutics, J Inst Bio, and Bayer within the past 36 months; got payment or honoraria for lectures or presentations from Pfizer, Janssen, Dava Oncology LLP, Caris Life Science and OncLive within the past 36 months; has received payment for scientific advisory board from Elevation Oncology within the past 36 months; and has stock ownership in MBrace Therapeutics, BlossomHill Therapeutics, Nuvalent, Lilly, Turning Point Therapeutics, and Elevation Oncology within the past 36 months. The authors have no other conflicts of interest to declare.
Figures


Similar articles
-
Low-Dose Computed Tomography (LDCT) Lung Cancer Screening in Asian Female Never-Smokers Is as Efficacious in Detecting Lung Cancer as in Asian Male Ever-Smokers: A Systematic Review and Meta-Analysis.J Thorac Oncol. 2023 Jun;18(6):698-717. doi: 10.1016/j.jtho.2023.01.094. Epub 2023 Feb 10. J Thorac Oncol. 2023. PMID: 36775191
-
Low-dose CT screening among never-smokers with or without a family history of lung cancer in Taiwan: a prospective cohort study.Lancet Respir Med. 2024 Feb;12(2):141-152. doi: 10.1016/S2213-2600(23)00338-7. Epub 2023 Nov 29. Lancet Respir Med. 2024. PMID: 38042167
-
Low-dose chest computed tomographic screening and invasive diagnosis of pulmonary nodules for lung cancer in never-smokers.Eur Respir J. 2020 Nov 12;56(5):2000177. doi: 10.1183/13993003.00177-2020. Print 2020 Nov. Eur Respir J. 2020. PMID: 32482786
-
Landscape on CT screening for lung cancer in Asia.Lung Cancer (Auckl). 2019 Sep 30;10:107-124. doi: 10.2147/LCTT.S192643. eCollection 2019. Lung Cancer (Auckl). 2019. PMID: 31686936 Free PMC article. Review.
-
Role of Low-Dose Computerized Tomography in Lung Cancer Screening among Never-Smokers.J Thorac Oncol. 2019 Mar;14(3):436-444. doi: 10.1016/j.jtho.2018.11.002. Epub 2018 Nov 13. J Thorac Oncol. 2019. PMID: 30445189 Clinical Trial.
Cited by
-
Impact of Race on the Outcomes of Retinoblastoma Treated With Primary Enucleation: A Global Study of 1426 Patients.Clin Exp Ophthalmol. 2025 May-Jun;53(4):421-434. doi: 10.1111/ceo.14488. Epub 2024 Dec 28. Clin Exp Ophthalmol. 2025. PMID: 39731391 Free PMC article.
References
-
- Force UPST. Final Recommendation Statement. Lung Cancer: Screening 2021. Available online: https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/lung...
LinkOut - more resources
Full Text Sources
Miscellaneous