

Development of a predictive model to predict postoperative bone metastasis in pathological I-II non-small cell lung cancer
- PMID: 38854951
- PMCID: PMC11157370
- DOI: 10.21037/tlcr-23-866
Development of a predictive model to predict postoperative bone metastasis in pathological I-II non-small cell lung cancer
Abstract
Background: Bone is a common metastatic site in postoperative metastasis, but related risk factors for early-stage non-small cell lung cancer (NSCLC) remain insufficiently investigated. Thus, the study aimed to identify risk factors for postoperative bone metastasis in early-stage NSCLC and construct a nomogram to identify high-risk individuals.
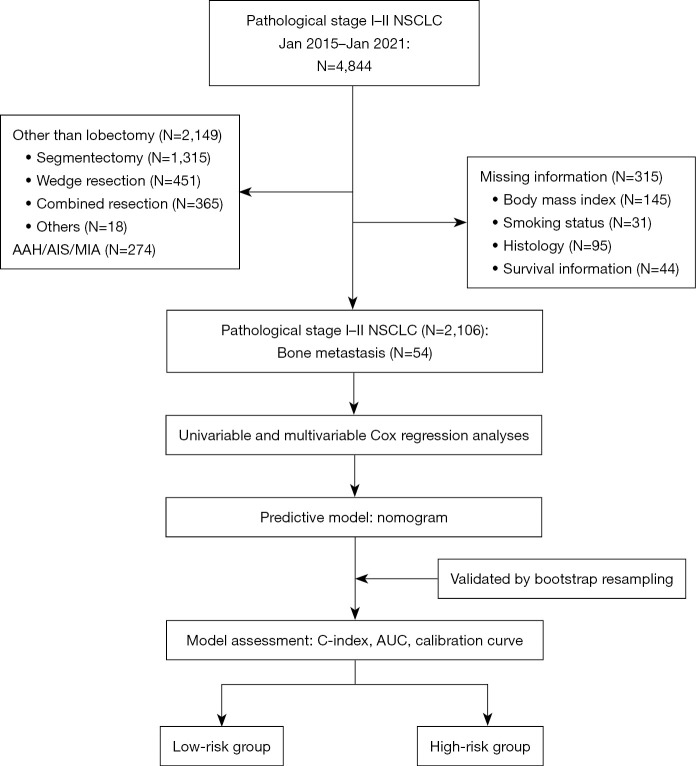
Methods: Between January 2015 and January 2021, we included patients with resected stage I-II NSCLC at the Department of Thoracic Surgery, West China Hospital. Univariable and multivariable Cox regression analyses were used to identify related risk factors. Additionally, we developed a visual nomogram to forecast the likelihood of bone metastasis. Evaluation of the model involved metrics such as the area under the curve (AUC), C-index, and calibration curves. To ensure reliability, internal validation was performed through bootstrap resampling.
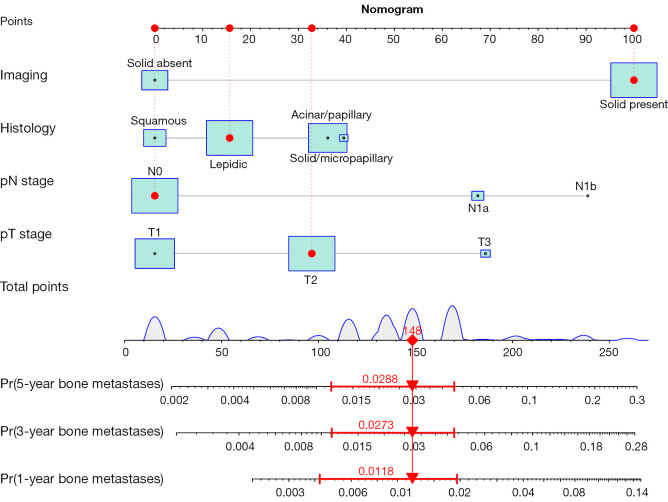
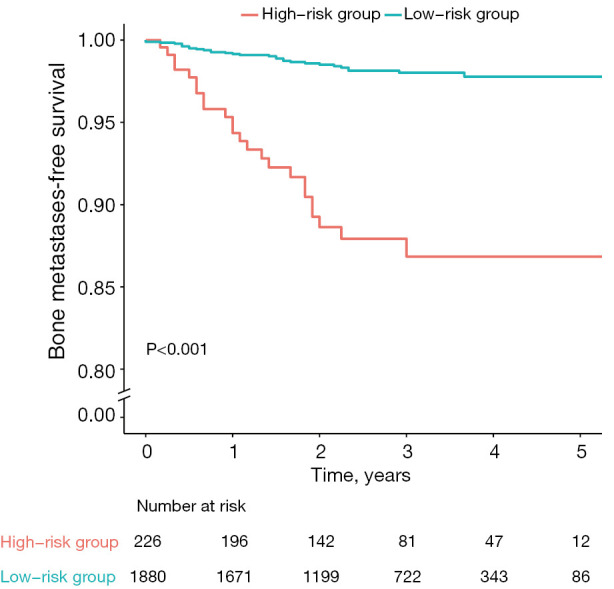
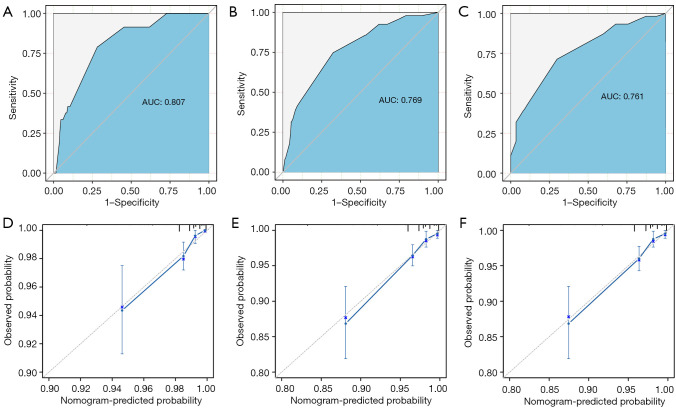
Results: Our analyses included 2,106 eligible patients, with 54 (2.56%) developing bone metastasis. Multivariable Cox analyses showed that tumor nodules with solid component, higher pT stage, higher pN stage, and histologic subtypes especially solid/micropapillary predominant types were considered as independent risk factors of bone metastasis. In the training set, the developed model demonstrated AUCs of 0.807, 0.769, and 0.761 for 1-, 3-, and 5-year follow-ups, respectively. The C-index, derived from 1,000 bootstrap resampling, showed values of 0.820, 0.793, and 0.777 for 1-, 3-, and 5-year follow-ups. The calibration curve showed that the model was well calibrated.
Conclusions: The predictive model is proven to be valuable in estimating the probability of bone metastasis in early-stage NSCLC following surgery. Leveraging four easy-to-acquire clinical parameters, this model effectively identifies high-risk patients and enables individualized surveillance strategies for better patient care.
Keywords: Early-stage non-small cell lung cancer (early-stage NSCLC); bone metastases; predictive model; risk factors.
2024 Translational Lung Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tlcr.amegroups.com/article/view/10.21037/tlcr-23-866/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
A clinical model to predict brain metastases in resected early-stage non-small cell lung cancer.BMC Cancer. 2025 Feb 11;25(1):236. doi: 10.1186/s12885-025-13609-y. BMC Cancer. 2025. PMID: 39934713 Free PMC article.
-
Development and validation of an early diagnosis model for bone metastasis in non-small cell lung cancer based on serological characteristics of the bone metastasis mechanism.EClinicalMedicine. 2024 Apr 26;72:102617. doi: 10.1016/j.eclinm.2024.102617. eCollection 2024 Jun. EClinicalMedicine. 2024. PMID: 38707910 Free PMC article.
-
A survival nomogram model for patients with resectable non-small cell lung cancer and lymph node metastasis (N1 or N2) based on the Surveillance, Epidemiology, and End Results Database and single-center data.Transl Lung Cancer Res. 2024 Mar 29;13(3):573-586. doi: 10.21037/tlcr-24-119. Epub 2024 Mar 27. Transl Lung Cancer Res. 2024. PMID: 38601448 Free PMC article.
-
Development and validation of a nomogram for predicting the overall survival in non-small cell lung cancer patients with liver metastasis.Transl Cancer Res. 2023 Nov 30;12(11):3061-3073. doi: 10.21037/tcr-23-899. Epub 2023 Oct 26. Transl Cancer Res. 2023. PMID: 38130305 Free PMC article.
-
Analysis of prognostic factors of metastatic endometrial cancer based on surveillance, epidemiology, and end results database.Front Surg. 2023 Jan 6;9:1001791. doi: 10.3389/fsurg.2022.1001791. eCollection 2022. Front Surg. 2023. PMID: 36684133 Free PMC article. Review.
Cited by
-
Risk factors and clinical risk stratification of distant metastasis in early-stage lung cancer in never smokers.World J Surg Oncol. 2025 Jun 18;23(1):238. doi: 10.1186/s12957-025-03892-1. World J Surg Oncol. 2025. PMID: 40533740 Free PMC article.
References
LinkOut - more resources
Full Text Sources