

Residual dizziness after BPPV management: exploring pathophysiology and treatment beyond canalith repositioning maneuvers
- PMID: 38854956
- PMCID: PMC11157684
- DOI: 10.3389/fneur.2024.1382196
Residual dizziness after BPPV management: exploring pathophysiology and treatment beyond canalith repositioning maneuvers
Erratum in
-
Corrigendum: Residual dizziness after BPPV management: exploring pathophysiology and treatment beyond canalith repositioning maneuvers.Front Neurol. 2024 Jul 29;15:1461600. doi: 10.3389/fneur.2024.1461600. eCollection 2024. Front Neurol. 2024. PMID: 39135752 Free PMC article.
Abstract
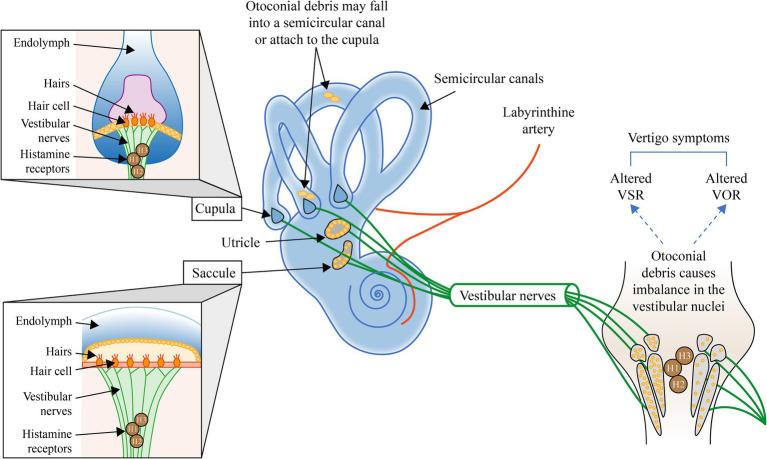
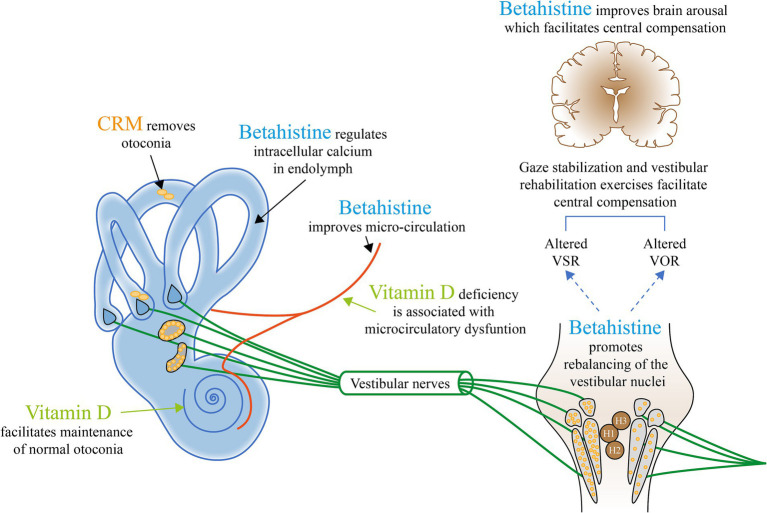
Despite the high success rate of canalith repositioning maneuvers (CRMs) in the treatment of benign paroxysmal positional vertigo (BPPV), a growing number of patients report residual dizziness symptoms that may last for a significant time. Although the majority of BPPV cases can be explained by canalolithiasis, the etiology is complex. Consideration of the individual patient's history and underlying pathophysiology of BPPV may offer the potential for treatment approaches supplementary to CRMs, as well as a promising alternative for patients in whom CRMs are contraindicated. This article provides a summary of the possible underlying causes of BPPV and residual dizziness, along with suggestions for potential management options that may be considered to relieve the burden of residual symptoms.
Keywords: benign paroxysmal positional vertigo; holistic; pathophysiology; residual dizziness; vestibular compensation.
Copyright © 2024 Özgirgin, Kingma, Manzari and Lacour.
Conflict of interest statement
The authors declare that this study received funding from Abbott Products Operations AG, Allschwil, Switzerland to provide editorial support for the development of the manuscript. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures

Similar articles
-
[Curative effect analysis of the vestibular rehabilitation training on residual dizziness after successful canalith repositioning maneuvers in patients with benign paroxysmal positional vertigo].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2017 Jun 20;31(12):897-900. doi: 10.13201/j.issn.1001-1781.2017.12.001. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2017. PMID: 29798407 Clinical Trial. Chinese.
-
Corrigendum: Residual dizziness after BPPV management: exploring pathophysiology and treatment beyond canalith repositioning maneuvers.Front Neurol. 2024 Jul 29;15:1461600. doi: 10.3389/fneur.2024.1461600. eCollection 2024. Front Neurol. 2024. PMID: 39135752 Free PMC article.
-
"Sitting-up vertigo as an expression of posterior semicircular canal heavy cupula and posterior semicircular canal short arm canalolithiasis".J Otol. 2022 Apr;17(2):101-106. doi: 10.1016/j.joto.2022.02.001. Epub 2022 Feb 16. J Otol. 2022. PMID: 35949549 Free PMC article.
-
Residual Dizziness after Successful Repositioning Maneuver for Idiopathic Benign Paroxysmal Positional Vertigo: A Review.Audiol Res. 2017 May 9;7(1):178. doi: 10.4081/audiores.2017.178. eCollection 2017 Feb 1. Audiol Res. 2017. PMID: 28603599 Free PMC article. Review.
-
[Challenge in the management of benign paroxysmal positional vertigo].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2016 Jul 20;30(14):1161-1163. doi: 10.13201/j.issn.1001-1781.2016.14.020. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2016. PMID: 29798448 Review. Chinese.
Cited by
-
Evaluating the efficacy of vestibular rehabilitation therapy on quality of life in persistent postural-perceptual dizziness: the role of anxiety and depression in treatment outcomes.Front Neurol. 2025 Feb 4;16:1524324. doi: 10.3389/fneur.2025.1524324. eCollection 2025. Front Neurol. 2025. PMID: 39968458 Free PMC article.
-
Machine Learning-Based Mobile Application for Predicting Posterior Canal Benign Paroxysmal Positional Vertigo.Laryngoscope Investig Otolaryngol. 2025 Jun 14;10(3):e70177. doi: 10.1002/lio2.70177. eCollection 2025 Jun. Laryngoscope Investig Otolaryngol. 2025. PMID: 40521132 Free PMC article.
-
Variations in the Diagnosis and Management of Benign Paroxysmal Positional Vertigo Among Physician Specialties in Saudi Arabia: Influence of Clinical Experience and Case Exposure.Healthcare (Basel). 2025 Aug 1;13(15):1887. doi: 10.3390/healthcare13151887. Healthcare (Basel). 2025. PMID: 40805918 Free PMC article.
-
Understanding Benign Paroxysmal Positional Vertigo (BPPV) and Its Impact on Quality of Life: A Systematic Review.Cureus. 2024 Jun 24;16(6):e63039. doi: 10.7759/cureus.63039. eCollection 2024 Jun. Cureus. 2024. PMID: 39050283 Free PMC article. Review.
-
Altered Hippocampal Subfields Functional Connectivity in Benign Paroxysmal Positional Vertigo Patients With Residual Dizziness: A Resting-State fMRI Study.CNS Neurosci Ther. 2024 Dec;30(12):e70175. doi: 10.1111/cns.70175. CNS Neurosci Ther. 2024. PMID: 39690894 Free PMC article.
References
-
- Palmeri R, Kumar A. Benign paroxysmal positional vertigo In: StatPearls. Treasure Island (FL): StatPearls Publishing; (2023). Available at: https://www.ncbi.nlm.nih.gov/books/NBK470308/ - PubMed
Publication types
LinkOut - more resources
Full Text Sources