

Incidence and Risk Factors for Retinal Detachment Following Pediatric Cataract Surgery
- PMID: 38855013
- PMCID: PMC11162630
- DOI: 10.2147/OPTH.S464005
Incidence and Risk Factors for Retinal Detachment Following Pediatric Cataract Surgery
Abstract
Background: Retinal detachment is a major postsurgical threat in pediatric cataract surgery; however, the effect of axial length remains unclear. This study aimed to assess the relationship between axial length and detachment risk in vulnerable patients.
Methods: This retrospective cohort study analyzed 132 eyes of 84 pediatric cataract surgery patients aged <20 years old. Axial length was measured preoperatively, and the incidence of retinal detachment was recorded over a median follow-up of 4 years. Logistic regression analysis was used to examine the axial length-detachment relationship.
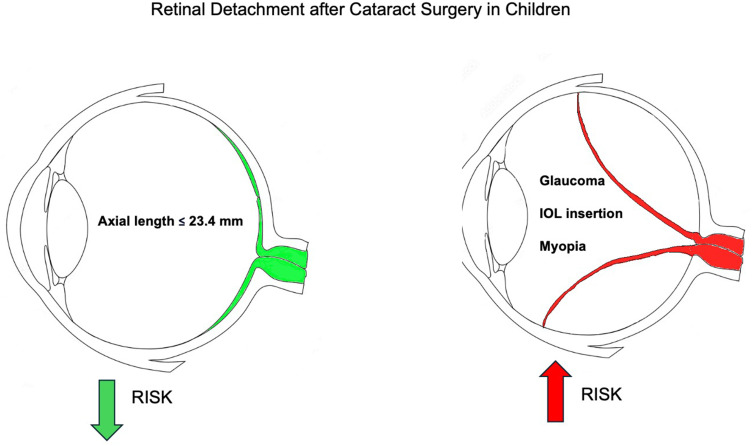
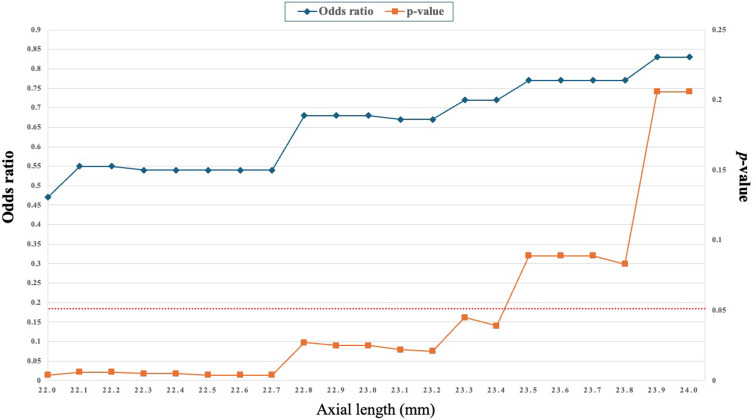
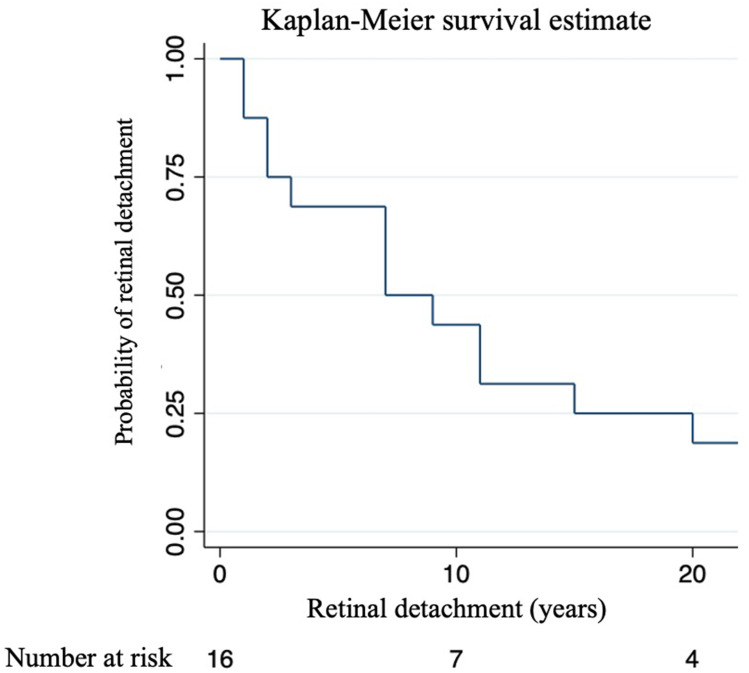
Results: Twenty eyes had postoperative retinal detachments. The median axial length was longer in the detachment group (23.6 mm) than in the non-detachment group (21.6 mm). Eyes with axial length ≤23.4 mm had 0.55-fold decreased odds of detachment compared to longer eyes. Preexisting myopia and glaucoma confer heightened risk. Approximately half of the patients retained some detachment risk eight years postoperatively.
Conclusion: Shorter eyes (axial length ≤23.4 mm) appear to be protected against pediatric retinal detachment after cataract surgery, whereas myopia, glaucoma, and axial elongation > 23.4 mm elevate the postoperative risk. Understanding these anatomical risk profiles requires surgical planning and follow-up care of children undergoing lensectomy.
Keywords: axial length; congenital cataract; congenital glaucoma; myopia; pediatric cataract surgery; retinal detachment.
Plain language summary
This study investigated the protective role of a shorter axial length in preventing retinal detachment after pediatric cataract surgery. This highlights the correlation between smaller eye sizes and reduced detachment risk, emphasizing the need for careful consideration of anatomical factors in surgical planning and patient monitoring, particularly for patients with preexisting myopia or postoperative glaucoma.
© 2024 Sabr et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Incidence, Risk Factors, and Outcomes of Retinal Detachment after Pediatric Cataract Surgery.Ophthalmology. 2018 Jan;125(1):36-42. doi: 10.1016/j.ophtha.2017.07.003. Epub 2017 Aug 24. Ophthalmology. 2018. PMID: 28844322
-
[Risk of retinal detachment in pseudophakia and axial myopia].Ophthalmologe. 1994 Dec;91(6):807-10. Ophthalmologe. 1994. PMID: 7849436 German.
-
Frequency of retinal detachment after cataract surgery in highly myopic patients.Saudi Med J. 2013 May;34(5):511-7. Saudi Med J. 2013. PMID: 23677268
-
Vitreous surgery for macular hole-related retinal detachment after phacoemulsification cataract extraction: 10-year retrospective review.Eye (Lond). 2012 Aug;26(8):1058-64. doi: 10.1038/eye.2012.87. Epub 2012 May 18. Eye (Lond). 2012. PMID: 22595907 Free PMC article. Review.
-
Retinal detachment following cataract phacoemulsification-a review of the literature.Eye (Lond). 2020 Apr;34(4):616-631. doi: 10.1038/s41433-019-0575-z. Epub 2019 Oct 1. Eye (Lond). 2020. PMID: 31576027 Free PMC article. Review.
Cited by
-
Factors Associated with Retinal Detachment after Pediatric Cataract Surgery in the IRIS® Registry.Ophthalmology. 2025 Aug;132(8):888-894. doi: 10.1016/j.ophtha.2025.03.003. Epub 2025 Mar 11. Ophthalmology. 2025. PMID: 40081617
References
LinkOut - more resources
Full Text Sources
