

Interfascial planes as surgical landmarks for laparoscopic upper retroperitoneal surgery: a cadaveric and retrospectively clinical study
- PMID: 38855604
- PMCID: PMC11157410
- DOI: 10.21037/tau-23-632
Interfascial planes as surgical landmarks for laparoscopic upper retroperitoneal surgery: a cadaveric and retrospectively clinical study
Abstract
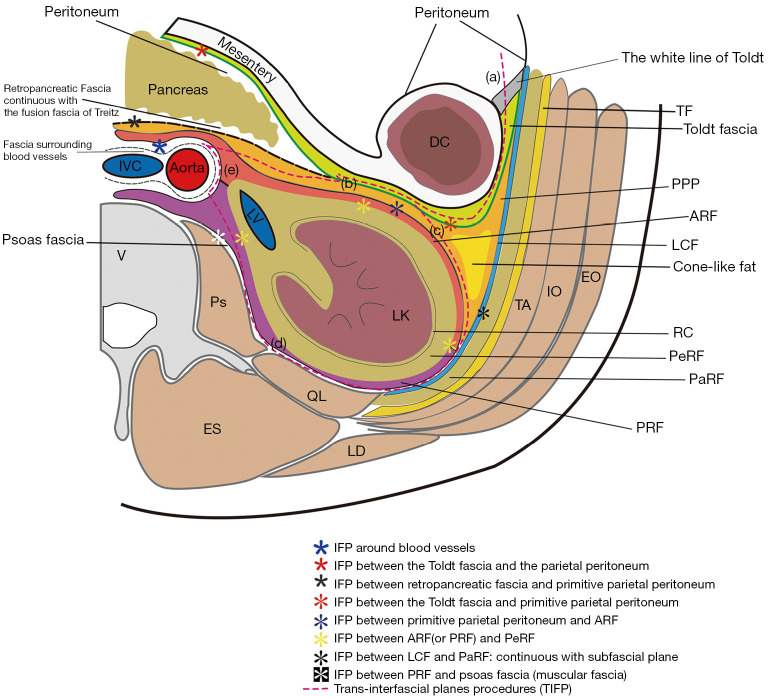
Background: Radiologists currently accept the concept of "interfascial plane (IFP)" to understand retroperitoneal anatomy, replacing Meyers' classic tricompartmental theory. Despite much research on retroperitoneal anatomy, its anatomical structure, embryonic origin and developmental process still require further exploration to guide the optimization of surgical process. This study aims to explore the anatomical basis of IFP related to laparoscopic upper retroperitoneal surgery (LURS) and to compare the clinical outcomes of trans-interfascial plane procedures for LURS (TIFP-LURS) with conventional LURS (Con-LURS).
Methods: The study consisted of two parts: cadaveric and clinical study. The cadaveric study involved dissecting and observing the retroperitoneal fasciae and IFP in 32 cadavers using gross anatomical and histological methods. This retrospective clinical study compared the perioperative data and complications of 229 patients who underwent TIFP-LURS and 121 patients who underwent Con-LURS for upper retroperitoneal lesions at our center.
Results: The cadaveric study revealed that the retroperitoneal space was composed of multilaminar fasciae that formed potential bloodless spaces among them, that could be used as surgical landmarks and operating planes. The clinical study showed that TIFP-LURS had a significantly less estimated blood loss, lower intraoperative complication rate, lower postoperative complication rate, shorter hospital-stay and lower long-term postoperative complications rate than Con-LURS. Multivariate analysis indicated that the TIFP procedure was an independent protective factor for decreasing the risk of postoperative complications.
Conclusions: The IFP are potential avascular spaces that can be used during laparoscopic surgery, and TIFP-LURS is a novel surgical approach that can improve the safety and efficacy of laparoscopic surgery for upper retroperitoneal lesions.
Keywords: Retroperitoneal anatomy; interfascial plane (IFP); laparoscopic upper retroperitoneal surgery (LURS).
2024 Translational Andrology and Urology. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tau.amegroups.com/article/view/10.21037/tau-23-632/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Preliminary embryological study of the radiological concept of retroperitoneal interfascial planes: what are the interfascial planes?Surg Radiol Anat. 2014 Dec;36(10):1079-87. doi: 10.1007/s00276-014-1301-y. Epub 2014 May 10. Surg Radiol Anat. 2014. PMID: 24817559
-
The retroperitoneal interfascial planes: current overview and future perspectives.Acute Med Surg. 2016 Feb 26;3(3):219-229. doi: 10.1002/ams2.188. eCollection 2016 Jul. Acute Med Surg. 2016. PMID: 29123789 Free PMC article. Review.
-
[Better understanding of interfacial planes in colorectal cancer surgery and the value of small vessels on fascia in the identification of interfacial planes].Zhonghua Wei Chang Wai Ke Za Zhi. 2020 Jul 25;23(7):670-675. doi: 10.3760/cma.j.cn.441530-20200508-00265. Zhonghua Wei Chang Wai Ke Za Zhi. 2020. PMID: 32683829 Chinese.
-
Safety and efficacy of laparoscopic transperitoneal versus retroperitoneal resection for benign retroperitoneal tumors: a retrospective cohort study.Surg Endosc. 2023 Dec;37(12):9299-9309. doi: 10.1007/s00464-023-10504-0. Epub 2023 Oct 26. Surg Endosc. 2023. PMID: 37884734
-
[Scientific interpretation of membrane anatomy theory and standardized application of membrane anatomy terms].Zhonghua Wei Chang Wai Ke Za Zhi. 2020 Jul 25;23(7):634-642. doi: 10.3760/cma.j.cn.441530-20200331-00177. Zhonghua Wei Chang Wai Ke Za Zhi. 2020. PMID: 32683822 Review. Chinese.
References
LinkOut - more resources
Full Text Sources