

From bone to nanoparticles: development of a novel generation of bone derived nanoparticles for image guided orthopedic regeneration
- PMID: 38856671
- PMCID: PMC11238765
- DOI: 10.1039/d4bm00391h
From bone to nanoparticles: development of a novel generation of bone derived nanoparticles for image guided orthopedic regeneration
Abstract
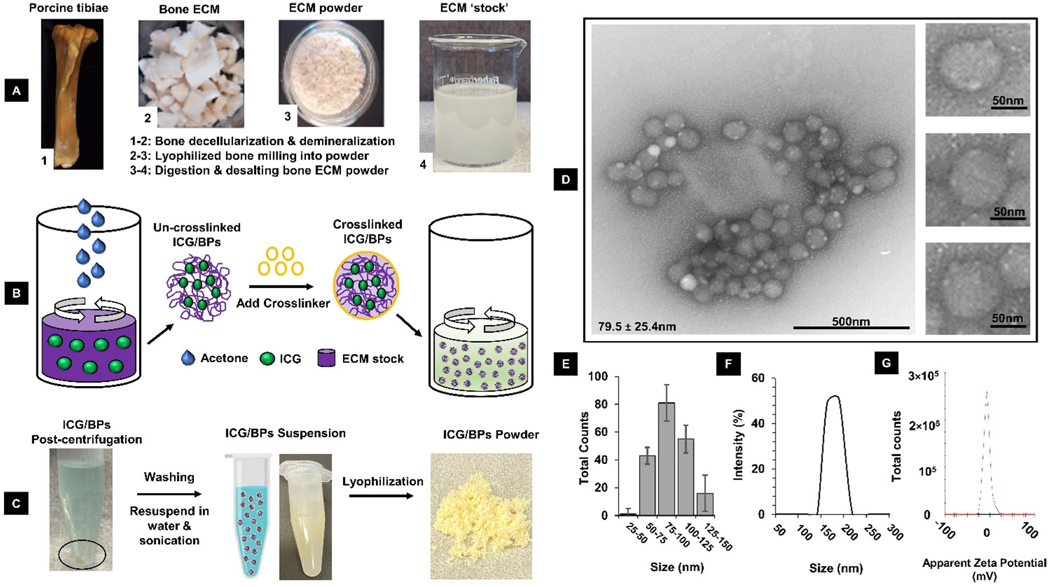
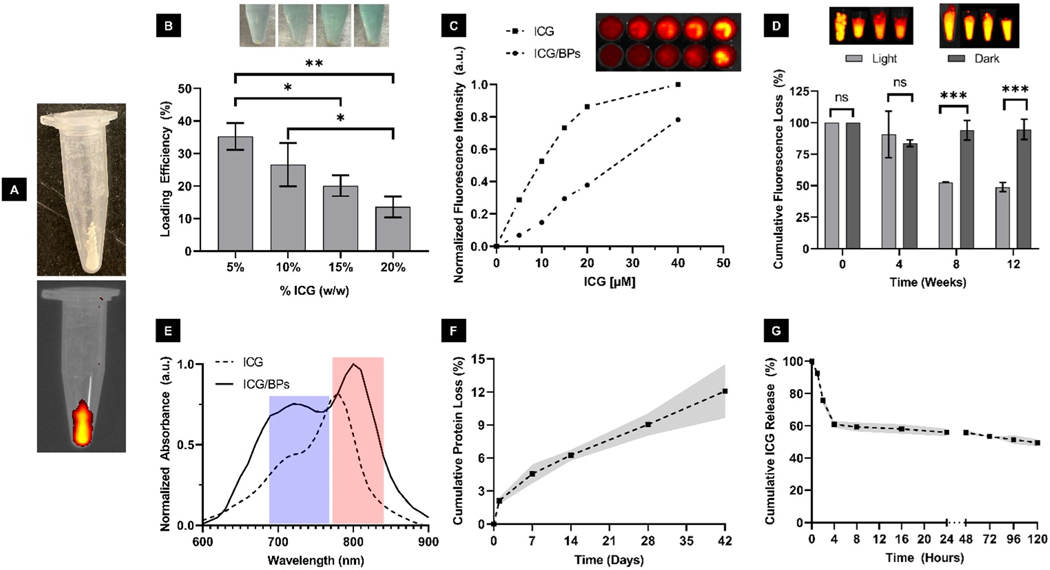
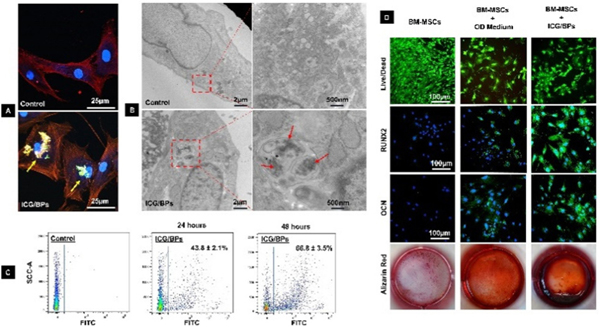
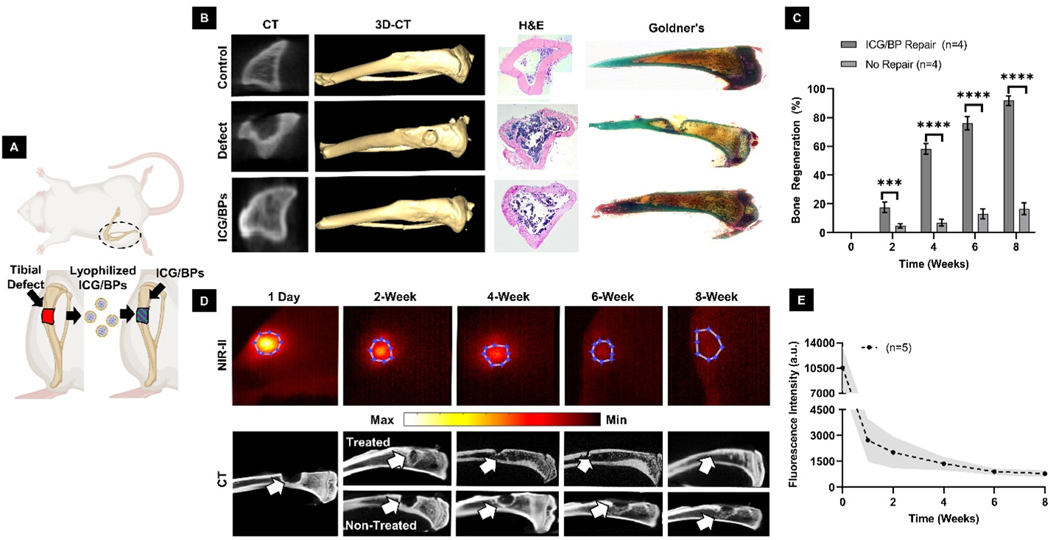
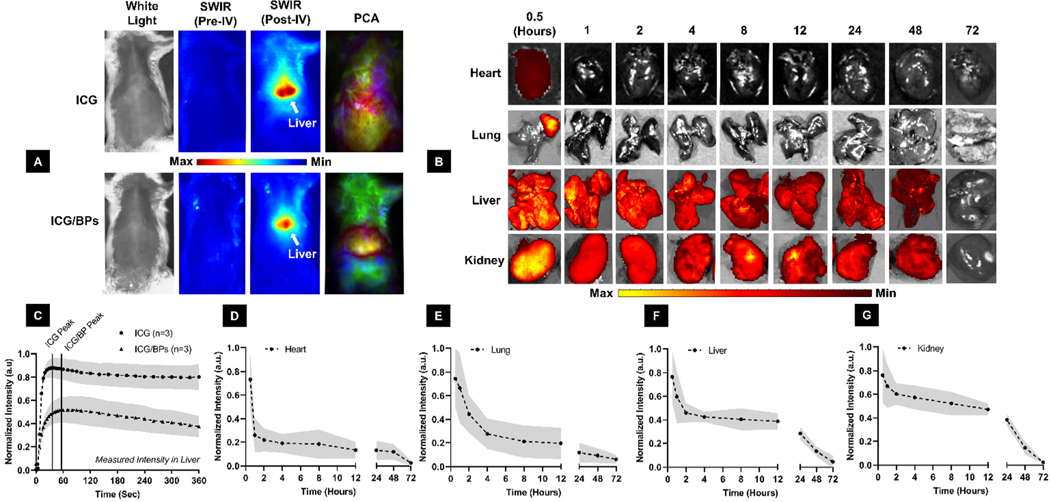
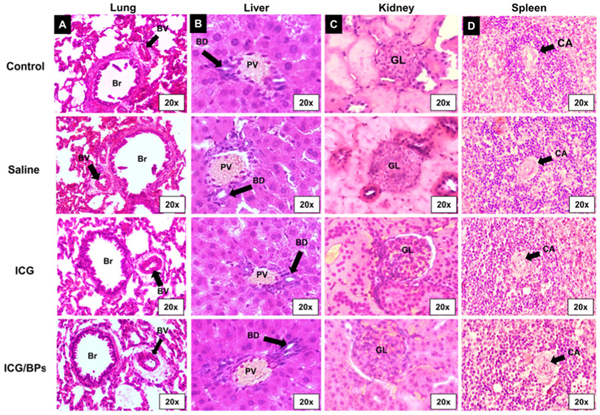
Bone related diseases such as osteoporosis, osteoarthritis, metastatic bone cancer, osteogenesis imperfecta, and Paget's disease, are primarily treated with pharmacologic therapies that often exhibit limited efficacy and substantial side effects. Bone injuries or fractures are primarily repaired with biocompatible materials that produce mixed results in sufficiently regenerating healthy and homogenous bone tissue. Each of these bone conditions, both localized and systemic, use different strategies with the same goal of achieving a healthy and homeostatic bone environment. In this study, we developed a new type of bone-based nanoparticle (BPs) using the entire organic extracellular matrix (ECM) of decellularized porcine bone, additionally encapsulating indocyanine green dye (ICG) for an in vivo monitoring capability. Utilizing the regenerative capability of bone ECM and the functionality of nanoparticles, the ICG encapsulated BPs (ICG/BPs) have been demonstrated to be utilized as a therapeutic option for localized and systemic orthopedic conditions. Additionally, ICG enables an in situ monitoring capability in the Short-Wave Infrared (SWIR) spectrum, capturing the degradation or the biodistribution of the ICG/BPs after both local implantation and intravenous administration, respectively. The efficacy and safety of the ICG/BPs shown within this study lay the foundation for future investigations, which will delve into optimization for clinical translation.
Conflict of interest statement
Conflicts of interest
The authors declare that they have no conflict of interest.
Figures
References
-
- Laurencin CT, Ambrosio AM, Borden MD and Cooper JA Jr., Annu. Rev. Biomed. Eng, 1999, 1, 19–46. - PubMed
-
- Bhatt RA and Rozental TD, Handb. Clin, 2012, 28, 457–468. - PubMed
-
- Lobb DC, DeGeorge BR Jr. and Chhabra AB, J. Hand Surg., Am., 2019, 44, 497–505.e2. - PubMed
-
- Rupp M, Klute L, Baertl S, Walter N, Mannala GK, Frank L, Pfeifer C, Alt V and Kerschbaum M, J. Biomed. Mater. Res., Part B, 2022, 110, 350–357. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources