

Atherosclerotic Cardiovascular Disease Risk Estimates Using the Predicting Risk of Cardiovascular Disease Events Equations
- PMID: 38856978
- PMCID: PMC11165411
- DOI: 10.1001/jamainternmed.2024.1302
Atherosclerotic Cardiovascular Disease Risk Estimates Using the Predicting Risk of Cardiovascular Disease Events Equations
Abstract
Importance: In 2023, the American Heart Association (AHA) developed the Predicting Risk of Cardiovascular Disease Events (PREVENT) equations to estimate 10-year risk of atherosclerotic cardiovascular disease (ASCVD), as an update to the 2013 pooled cohort equations (PCEs). The PREVENT equations were derived from contemporary cohorts and removed race and added variables for kidney function and statin use.
Objective: To compare national estimates of 10-year ASCVD risk using the PCEs and PREVENT equations and how these equations affect recommendations for primary prevention statin therapy.
Design, setting, and participants: This cross-sectional study included adults aged 40 to 75 years who participated in the National Health and Nutrition Examination Survey from 2017 to March 2020. Adults were defined as eligible for primary prevention statin use based on the 2019 AHA/American College of Cardiology guideline on the primary prevention of cardiovascular disease. Data were weighted to be nationally representative and were analyzed from December 27, 2023, to January 31, 2024.
Main outcomes and measures: The 10-year ASCVD risk and eligibility for primary prevention statin therapy based on PREVENT and PCE calculations.
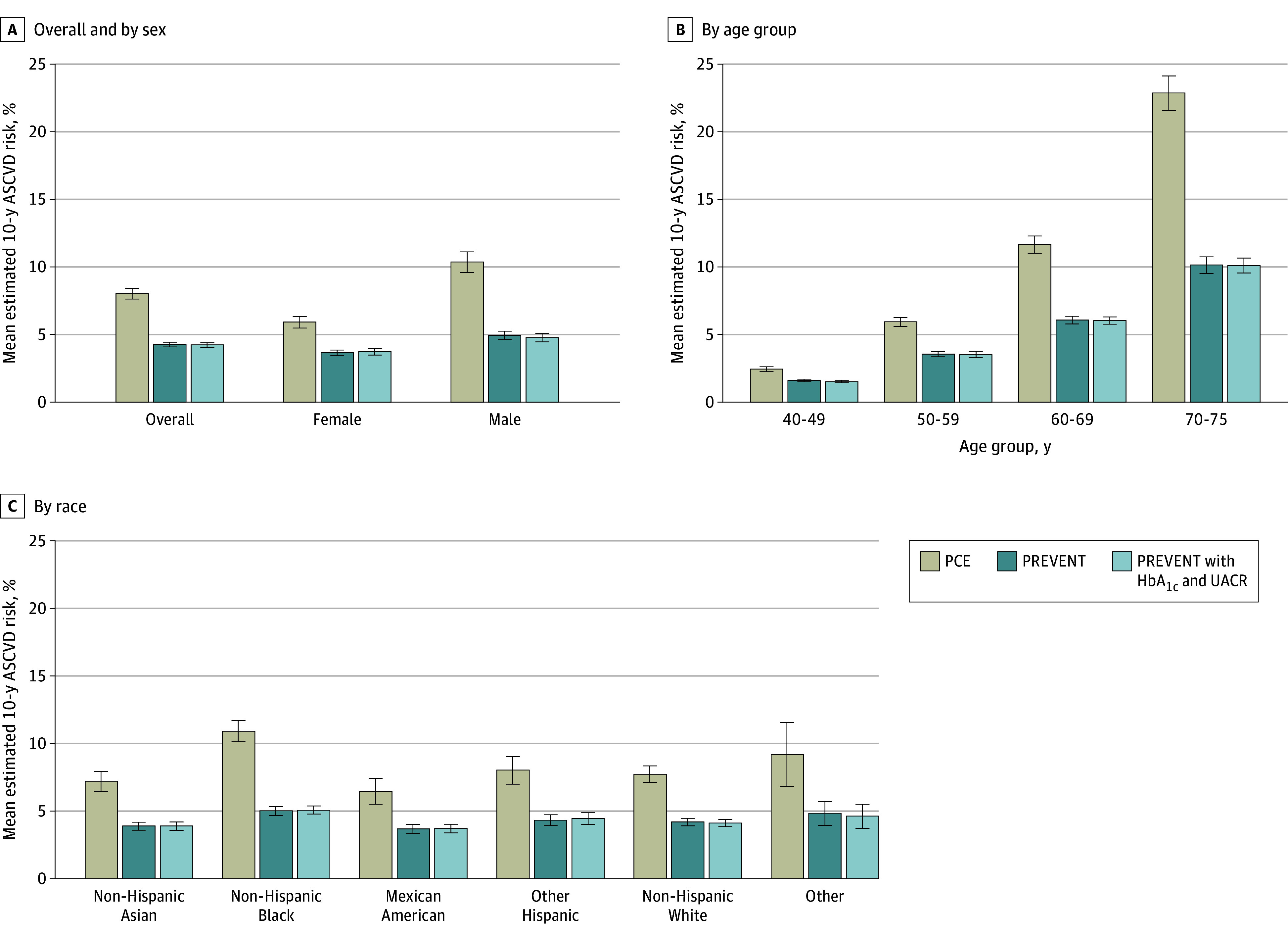
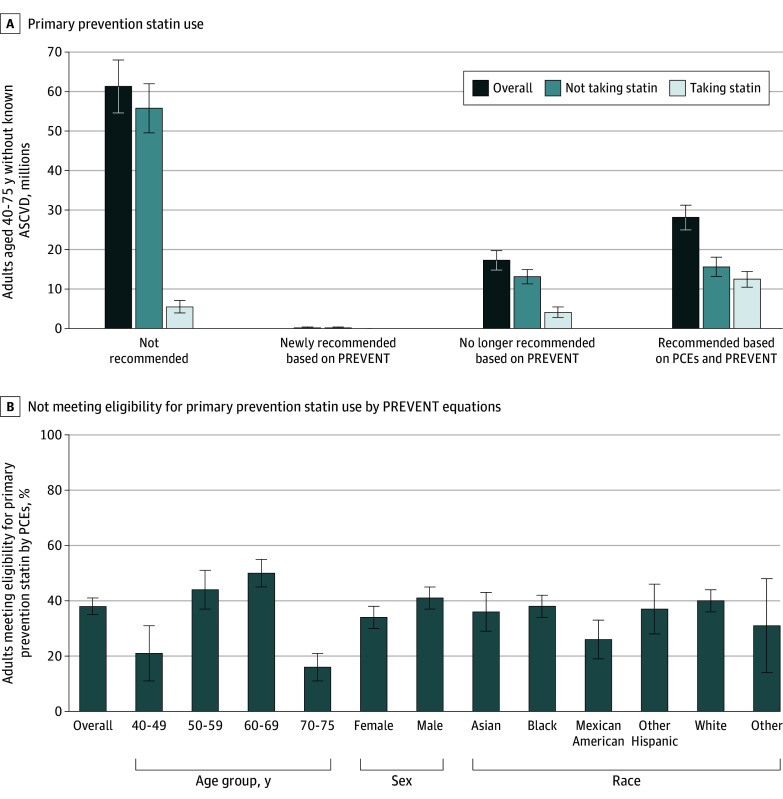
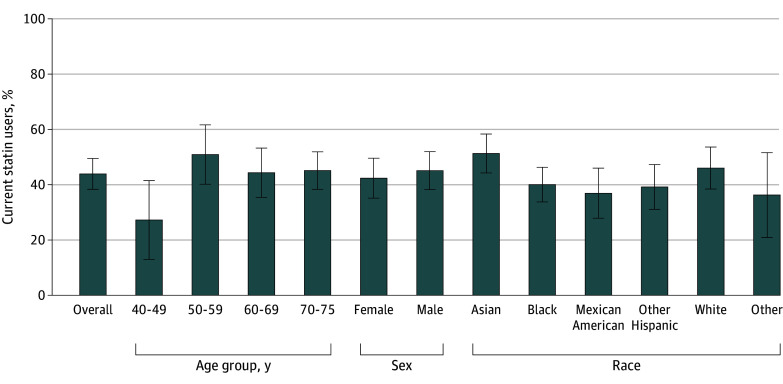
Results: In the weighted sample of 3785 US adults (mean [SD] age, 55.7 [9.7] years; 52.5% women) without known ASCVD, 20.7% reported current statin use. The mean estimated 10-year ASCVD risk was 8.0% (95% CI, 7.6%-8.4%) using the PCEs and 4.3% (95% CI, 4.1%-4.5%) using the PREVENT equations. Across all age, sex, and racial subgroups, compared with the PCEs, the mean estimated 10-year ASCVD risk was lower using the PREVENT equations, with the largest difference for Black adults (10.9% [95% CI, 10.1%-11.7%] vs 5.1% [95% CI 4.7%-5.4%]) and individuals aged 70 to 75 years (22.8% [95% CI, 21.6%-24.1%] vs 10.2% [95% CI, 9.6%-10.8%]). The use of the PREVENT equations instead of the PCEs could reduce the number of adults meeting criteria for primary prevention statin therapy from 45.4 million (95% CI, 40.3 million-50.4 million) to 28.3 million (95% CI, 25.2 million-31.4 million). In other words, 17.3 million (95% CI, 14.8 million-19.7 million) adults recommended statins based on the PCEs would no longer be recommended statins based on PREVENT equations, including 4.1 million (95% CI, 2.8 million-5.5 million) adults currently taking statins. Based on the PREVENT equations, 44.1% (95% CI, 38.6%-49.5%) of adults eligible for primary prevention statin therapy reported currently taking statins, equating to 15.8 million (95% CI, 13.4 million-18.2 million) individuals eligible for primary prevention statins who reported not taking statins.
Conclusions and relevance: This cross-sectional study found that use of the PREVENT equations was associated with fewer US adults being eligible for primary prevention statin therapy; however, the majority of adults eligible for receiving such therapy based on PREVENT equations did not report statin use.
Conflict of interest statement
Figures
References
-
- Goff DC Jr, Lloyd-Jones DM, Bennett G, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25, pt B):2935-2959. doi: 10.1016/j.jacc.2013.11.005 - DOI - PMC - PubMed
-
- DeFilippis AP, Young R, McEvoy JW, et al. Risk score overestimation: the impact of individual cardiovascular risk factors and preventive therapies on the performance of the American Heart Association-American College of Cardiology-Atherosclerotic Cardiovascular Disease risk score in a modern multi-ethnic cohort. Eur Heart J. 2017;38(8):598-608. doi: 10.1093/eurheartj/ehw301 - DOI - PMC - PubMed
-
- Khan SS, Matshushita K, Sang Y, et al. ; Chronic Kidney Disease Consortium and the American Heart Association Cardiovascular-Kidney-Metabolic Science Advisory Group . Development and validation of the American Heart Association’s PREVENT equations. Circulation. 2024;149(6):430-449.https://pubmed.ncbi.nlm.nih.gov/37947085 doi: 10.1161/CIRCULATIONAHA.123.067626 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
