

Lung Cancer Screening in the US, 2022
- PMID: 38856988
- PMCID: PMC11165414
- DOI: 10.1001/jamainternmed.2024.1655
Lung Cancer Screening in the US, 2022
Abstract
Importance: The US Preventive Services Task Force (USPSTF) recommends annual lung cancer screening (LCS) with low-dose computed tomography in high-risk individuals (age 50-80 years, ≥20 pack-years currently smoking or formerly smoked, and quit <15 years ago) for early detection of LC. However, representative state-level LCS data are unavailable nationwide.
Objective: To estimate the contemporary prevalence of up-to-date (UTD) LCS in the US nationwide and across the 50 states and the District of Columbia.
Design, setting, and participants: This cross-sectional study used data from the 2022 Behavioral Risk Factor Surveillance System (BRFSS) population-based, nationwide, state-representative survey for respondents aged 50 to 79 years who were eligible for LCS according to the 2021 USPSTF eligibility criteria. Data analysis was performed from October 1, 2023, to March 20, 2024.
Main outcomes and measures: The main outcome was self-reported UTD-LCS (defined as past-year) prevalence according to the 2021 USPSTF eligibility criteria in respondents aged 50 to 79 years. Adjusted prevalence ratios (APRs) and 95% CIs compared differences.
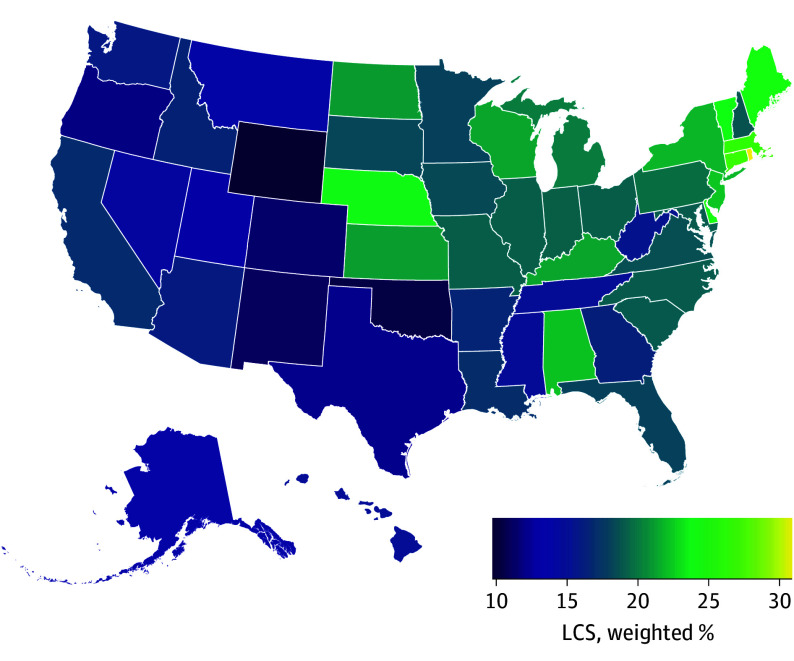
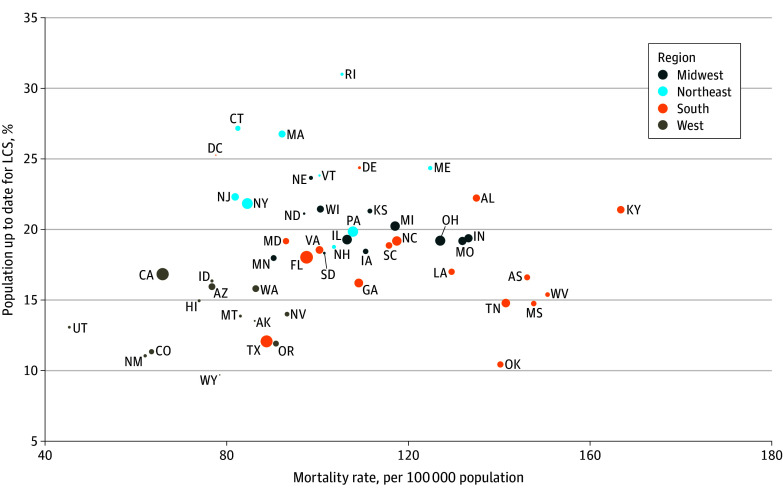
Results: Among 25 958 sample respondents eligible for LCS (median [IQR] age, 62 [11] years), 61.5% reported currently smoking, 54.4% were male, 64.4% were aged 60 years or older, and 53.0% had a high school education or less. The UTD-LCS prevalence was 18.1% overall, but varied across states (range, 9.7%-31.0%), with relatively lower levels in southern states characterized by high LC mortality burden. The UTD-LCS prevalence increased with age (50-54 years: 6.7%; 70-79 years: 27.1%) and number of comorbidities (≥3: 24.6%; none: 8.7%). A total of 3.7% of those without insurance and 5.1% of those without a usual source of care were UTD with LCS, but state-level Medicaid expansions (APR, 2.68; 95% CI, 1.30-5.53) and higher screening capacity levels (high vs low: APR, 1.93; 95% CI, 1.36-2.75) were associated with higher UTD-LCS prevalence.
Conclusions and relevance: This study of data from the 2022 BRFSS found that the overall prevalence of UTD-LCS was low. Disparities were largest according to health care access and geographically across US states, with low prevalence in southern states with high LC burden. The findings suggest that state-based initiatives to expand access to health care and screening facilities may be associated with improved LCS rates and reduced disparities.
Conflict of interest statement
Figures
Comment in
-
Progress in Lung Cancer Screening Adoption.JAMA Intern Med. 2024 Aug 1;184(8):902-903. doi: 10.1001/jamainternmed.2024.1673. JAMA Intern Med. 2024. PMID: 38857025 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
