

Intraoperative near infrared functional imaging of rectal cancer using artificial intelligence methods - now and near future state of the art
- PMID: 38858280
- PMCID: PMC11300525
- DOI: 10.1007/s00259-024-06731-9
Intraoperative near infrared functional imaging of rectal cancer using artificial intelligence methods - now and near future state of the art
Abstract
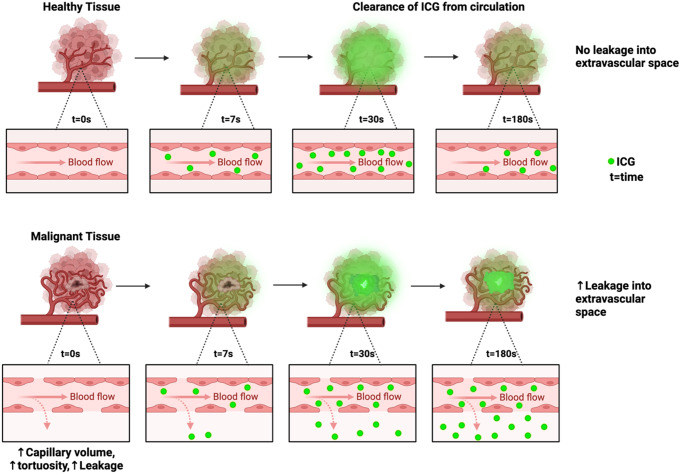
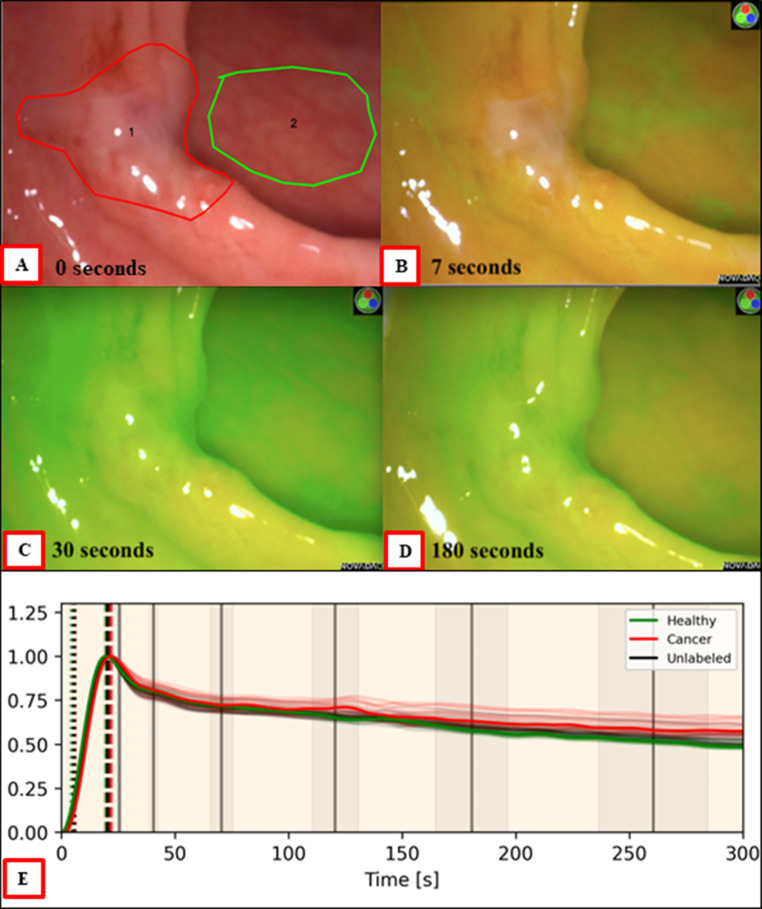
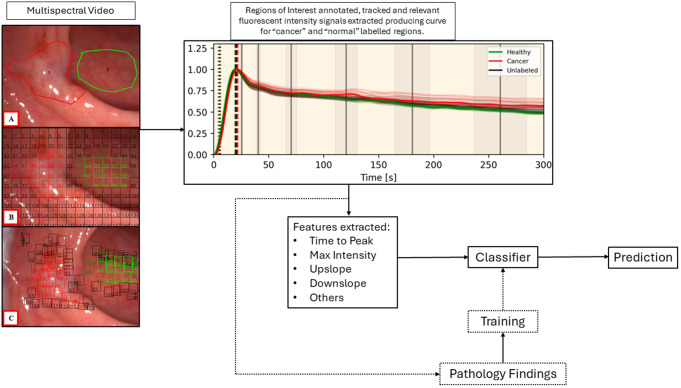
Colorectal cancer remains a major cause of cancer death and morbidity worldwide. Surgery is a major treatment modality for primary and, increasingly, secondary curative therapy. However, with more patients being diagnosed with early stage and premalignant disease manifesting as large polyps, greater accuracy in diagnostic and therapeutic precision is needed right from the time of first endoscopic encounter. Rapid advancements in the field of artificial intelligence (AI), coupled with widespread availability of near infrared imaging (currently based around indocyanine green (ICG)) can enable colonoscopic tissue classification and prognostic stratification for significant polyps, in a similar manner to contemporary dynamic radiological perfusion imaging but with the advantage of being able to do so directly within interventional procedural time frames. It can provide an explainable method for immediate digital biopsies that could guide or even replace traditional forceps biopsies and provide guidance re margins (both areas where current practice is only approximately 80% accurate prior to definitive excision). Here, we discuss the concept and practice of AI enhanced ICG perfusion analysis for rectal cancer surgery while highlighting recent and essential near-future advancements. These include breakthrough developments in computer vision and time series analysis that allow for real-time quantification and classification of fluorescent perfusion signals of rectal cancer tissue intraoperatively that accurately distinguish between normal, benign, and malignant tissues in situ endoscopically, which are now undergoing international prospective validation (the Horizon Europe CLASSICA study). Next stage advancements may include detailed digital characterisation of small rectal malignancy based on intraoperative assessment of specific intratumoral fluorescent signal pattern. This could include T staging and intratumoral molecular process profiling (e.g. regarding angiogenesis, differentiation, inflammatory component, and tumour to stroma ratio) with the potential to accurately predict the microscopic local response to nonsurgical treatment enabling personalised therapy via decision support tools. Such advancements are also applicable to the next generation fluorophores and imaging agents currently emerging from clinical trials. In addition, by providing an understandable, applicable method for detailed tissue characterisation visually, such technology paves the way for acceptance of other AI methodology during surgery including, potentially, deep learning methods based on whole screen/video detailing.
Keywords: Artificial intelligence; Clinical trials; Digital surgery; Dynamic imaging; Fluorescence guided surgery (FGS); Indocyanine green; Intraoperative imaging; Rectal cancer.
© 2024. The Author(s).
Conflict of interest statement
Ronan Cahill receives speaker fees from Stryker, Olympus, Ethicon and provides paid consultancy to Diagnostic Green, Arthrex and Medtronic. He also holds research funding from Intuitive Corp, and with IBM Research, Palliare and Arthrex from the Irish Government and the European Union as well as being a member of the medical advisory board of Palliare. Patrick Boland and Philip McEntee’s roles as research fellows are funded by the Horizon Europe CLASSICA Study and the European Union. Niall Hardy, Alice Moynihan, Caitlyn Loo and Helen Fenlon have no competing interests to declare.
Figures
Similar articles
-
A novel flexible near-infrared endoscopic device that enables real-time artificial intelligence fluorescence tissue characterization.PLoS One. 2025 Mar 13;20(3):e0317771. doi: 10.1371/journal.pone.0317771. eCollection 2025. PLoS One. 2025. PMID: 40080492 Free PMC article.
-
Technical and functional design considerations for a real-world interpretable AI solution for NIR perfusion analysis (including cancer).Eur J Surg Oncol. 2024 Dec;50(12):108273. doi: 10.1016/j.ejso.2024.108273. Epub 2024 Mar 18. Eur J Surg Oncol. 2024. PMID: 38538505 Review.
-
Near-Infrared Indocyanine Green-Enhanced Fluorescence and Minimally Invasive Colorectal Surgery: Review of the Literature.Surg Technol Int. 2018 Nov 11;33:77-83. Surg Technol Int. 2018. PMID: 30029290 Review.
-
Intraoperative use of indocyanine green fluorescence imaging in rectal cancer surgery: The state of the art.World J Gastroenterol. 2021 Oct 14;27(38):6374-6386. doi: 10.3748/wjg.v27.i38.6374. World J Gastroenterol. 2021. PMID: 34720528 Free PMC article. Review.
-
How to reduce surgical complications in rectal cancer surgery using fluorescence techniques.Minerva Chir. 2018 Apr;73(2):210-216. doi: 10.23736/S0026-4733.18.07632-0. Epub 2018 Feb 21. Minerva Chir. 2018. PMID: 29471617 Review.
Cited by
-
Fluorescence-Guided Surgery in Metabolic and Bariatric Surgery: Current Status and Future Directions.Obes Surg. 2025 Jul 22. doi: 10.1007/s11695-025-08111-0. Online ahead of print. Obes Surg. 2025. PMID: 40696086 No abstract available.
-
Recent Advances in Indocyanine Green-Based Probes for Second Near-Infrared Fluorescence Imaging and Therapy.Research (Wash D C). 2025 Jan 17;8:0583. doi: 10.34133/research.0583. eCollection 2025. Research (Wash D C). 2025. PMID: 39830366 Free PMC article. Review.
-
ICG fluorescence-guided sentinel lymph node biopsy for decision-making in lateral lymph node dissection in local advanced rectal cancer: a retrospective study.Updates Surg. 2025 Apr 9. doi: 10.1007/s13304-025-02169-2. Online ahead of print. Updates Surg. 2025. PMID: 40205080
-
Intraoperative quantitative analysis of intestinal perfusion by ICG fluorescence in Hirschsprung disease: a single-center retrospective cohort study.Pediatr Surg Int. 2025 Jul 23;41(1):227. doi: 10.1007/s00383-025-06068-w. Pediatr Surg Int. 2025. PMID: 40699330
-
Artificial Intelligence in Surgery: A Systematic Review of Use and Validation.J Clin Med. 2024 Nov 24;13(23):7108. doi: 10.3390/jcm13237108. J Clin Med. 2024. PMID: 39685566 Free PMC article. Review.
References
-
- Siegel RL, et al. Colorectal cancer statistics, 2023. CA Cancer J Clin. 2023;73(3):233–54. - PubMed
-
- Sung H, et al. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and Mortality Worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49. - PubMed
-
- Giuliani A, et al. Large size, villous content and distal location are associated with severe dysplasia in colorectal adenomas. Anticancer Res. 2006;26(5B):3717–22. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
