

Longitudinal neurofunctional changes in medication overuse headache patients after mindfulness practice in a randomized controlled trial (the MIND-CM study)
- PMID: 38858629
- PMCID: PMC11165872
- DOI: 10.1186/s10194-024-01803-5
Longitudinal neurofunctional changes in medication overuse headache patients after mindfulness practice in a randomized controlled trial (the MIND-CM study)
Abstract
Background: Mindfulness practice has gained interest in the management of Chronic Migraine associated with Medication Overuse Headache (CM-MOH). Mindfulness is characterized by present-moment self-awareness and relies on attention control and emotion regulation, improving headache-related pain management. Mindfulness modulates the Default Mode Network (DMN), Salience Network (SN), and Fronto-Parietal Network (FPN) functional connectivity. However, the neural mechanisms underlying headache-related pain management with mindfulness are still unclear. In this study, we tested neurofunctional changes after mindfulness practice added to pharmacological treatment as usual in CM-MOH patients.
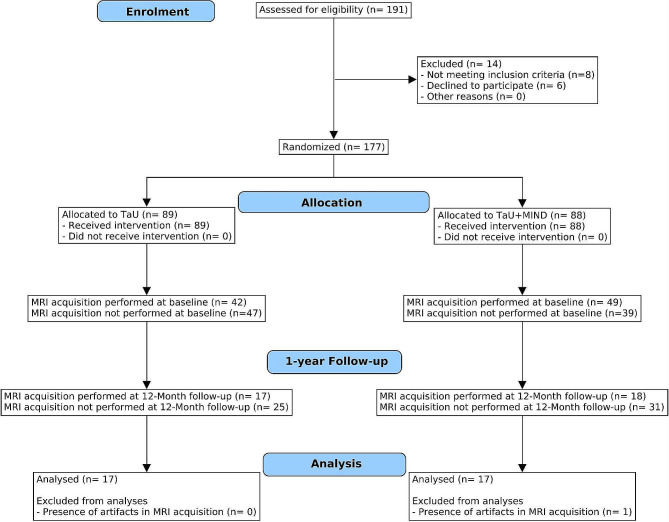
Methods: The present study is a longitudinal phase-III single-blind Randomized Controlled Trial (MIND-CM study; NCT03671681). Patients had a diagnosis of CM-MOH, no history of neurological and severe psychiatric comorbidities, and were attending our specialty headache centre. Patients were divided in Treatment as Usual (TaU) and mindfulness added to TaU (TaU + MIND) groups. Patients underwent a neuroimaging and clinical assessment before the treatment and after one year. Longitudinal comparisons of DMN, SN, and FPN connectivity were performed between groups and correlated with clinical changes. Vertex-wise analysis was performed to assess cortical thickness changes.
Results: 177 CM-MOH patients were randomized to either TaU group or TaU + MIND group. Thirty-four patients, divided in 17 TaU and 17 TaU + MIND, completed the neuroimaging follow-up. At the follow-up, both groups showed an improvement in most clinical variables, whereas only TaU + MIND patients showed a significant headache frequency reduction (p = 0.028). After one year, TaU + MIND patients showed greater SN functional connectivity with the left posterior insula (p-FWE = 0.007) and sensorimotor cortex (p-FWE = 0.026). In TaU + MIND patients only, greater SN-insular connectivity was associated with improved depression scores (r = -0.51, p = 0.038). A longitudinal increase in cortical thickness was observed in the insular cluster in these patients (p = 0.015). Increased anterior cingulate cortex thickness was also reported in TaU + MIND group (p-FWE = 0.02).
Conclusions: Increased SN-insular connectivity might modulate chronic pain perception and the management of negative emotions. Enhanced SN-sensorimotor connectivity could reflect improved body-awareness of painful sensations. Expanded cingulate cortex thickness might sustain improved cognitive processing of nociceptive information. Our findings unveil the therapeutic potential of mindfulness and the underlying neural mechanisms in CM-MOH patients.
Trial registration: Name of Registry; MIND-CM study; Registration Number ClinicalTrials.gov identifier: NCT0367168; Registration Date: 14/09/2018.
Keywords: Chronic pain; Cortical thickness; Functional connectivity; Headache; Medication overuse headache; Migraine; Mindfulness; Pain management; Resting state fMRI; Salience network.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests. AR is associate editor of The Journal of Headache and Pain. He was not involved in the journal’s peer review process of, or decisions related to, this manuscript.
Figures


Similar articles
-
Efficacy of mindfulness added to treatment as usual in patients with chronic migraine and medication overuse headache: a phase-III single-blind randomized-controlled trial (the MIND-CM study).J Headache Pain. 2023 Jul 14;24(1):86. doi: 10.1186/s10194-023-01630-0. J Headache Pain. 2023. PMID: 37452281 Free PMC article. Clinical Trial.
-
Neurotransmitter-related functional connectivity changes in serotonin and dopamine systems after mindfulness in medication overuse headache.Cephalalgia. 2025 Jun;45(6):3331024251332561. doi: 10.1177/03331024251332561. Epub 2025 Jun 8. Cephalalgia. 2025. PMID: 40485203
-
Resting State Functional Connectivity After Sphenopalatine Ganglion Blocks in Chronic Migraine With Medication Overuse Headache: A Pilot Longitudinal fMRI Study.Headache. 2018 May;58(5):732-743. doi: 10.1111/head.13318. Headache. 2018. PMID: 29878344
-
Resting-state fMRI functional connectivity and mindfulness in clinical and non-clinical contexts: A review and synthesis.Neurosci Biobehav Rev. 2022 Apr;135:104583. doi: 10.1016/j.neubiorev.2022.104583. Epub 2022 Feb 22. Neurosci Biobehav Rev. 2022. PMID: 35202647 Free PMC article. Review.
-
Meta-analytic evidence that mindfulness training alters resting state default mode network connectivity.Sci Rep. 2022 Jul 18;12(1):12260. doi: 10.1038/s41598-022-15195-6. Sci Rep. 2022. PMID: 35851275 Free PMC article.
Cited by
-
fMRI-based explanations for how meditation could modulate pain processing.Front Neurosci. 2025 May 16;19:1561580. doi: 10.3389/fnins.2025.1561580. eCollection 2025. Front Neurosci. 2025. PMID: 40454249 Free PMC article.
-
Psychopathological variables in chronic migraine patients with different therapeutic approach: psychological profile differences and impact on therapeutic efficacy in real life.Neurol Sci. 2024 Dec;45(12):5813-5821. doi: 10.1007/s10072-024-07769-1. Epub 2024 Sep 19. Neurol Sci. 2024. PMID: 39298029
-
Abnormal alterations in structure-function coupling at the modular level in patients with postherpetic neuralgia.Sci Rep. 2025 Jan 18;15(1):2377. doi: 10.1038/s41598-025-86908-w. Sci Rep. 2025. PMID: 39827190 Free PMC article.
-
Dropout Rate of Participants in Randomized Controlled Trials Using Different Exercise-Based Interventions in Patients with Migraine. A Systematic Review with Meta-Analysis.Healthcare (Basel). 2025 May 5;13(9):1061. doi: 10.3390/healthcare13091061. Healthcare (Basel). 2025. PMID: 40361839 Free PMC article. Review.
-
Assessment of hypothalamic macrostructure in episodic cluster headache: a volumetric segmentation MRI study.Radiol Med. 2025 Jun 27. doi: 10.1007/s11547-025-02041-8. Online ahead of print. Radiol Med. 2025. PMID: 40576879
References
Publication types
MeSH terms
Grants and funding
- National Recovery and Resilience Plan (NRRP), Mission 4 Component 2 Investment 3.3 - Call for tender No. 117 of 02/03/2023 of Italian Ministry of University and Research/European Union - NextGenerationEU
- RRC/Ministero della Salute
- RF-2016-02364801/Ministero della Salute
- RRC/Ministero della Salute
- RRC/Ministero della Salute
LinkOut - more resources
Full Text Sources
