

Adverse events at the end of life of hospital patients with or without a condition relevant for palliative care: a nationwide retrospective record review study in the Netherlands
- PMID: 38858703
- PMCID: PMC11163706
- DOI: 10.1186/s12904-024-01461-z
Adverse events at the end of life of hospital patients with or without a condition relevant for palliative care: a nationwide retrospective record review study in the Netherlands
Abstract
Background: Patient safety is crucial for quality of care. Preventable adverse events (AEs) occur in 1 of 20 patients in the hospital, but it is unknown whether this is different for patients with a condition relevant for palliative care. The majority of the limited available research on this topic is only focused on patients already receiving palliative care, and do not make comparisons with other patients at the end-of-life. We identified and compared the prevalence, preventability, nature and causes of AEs in patients with and without a condition relevant for palliative care.
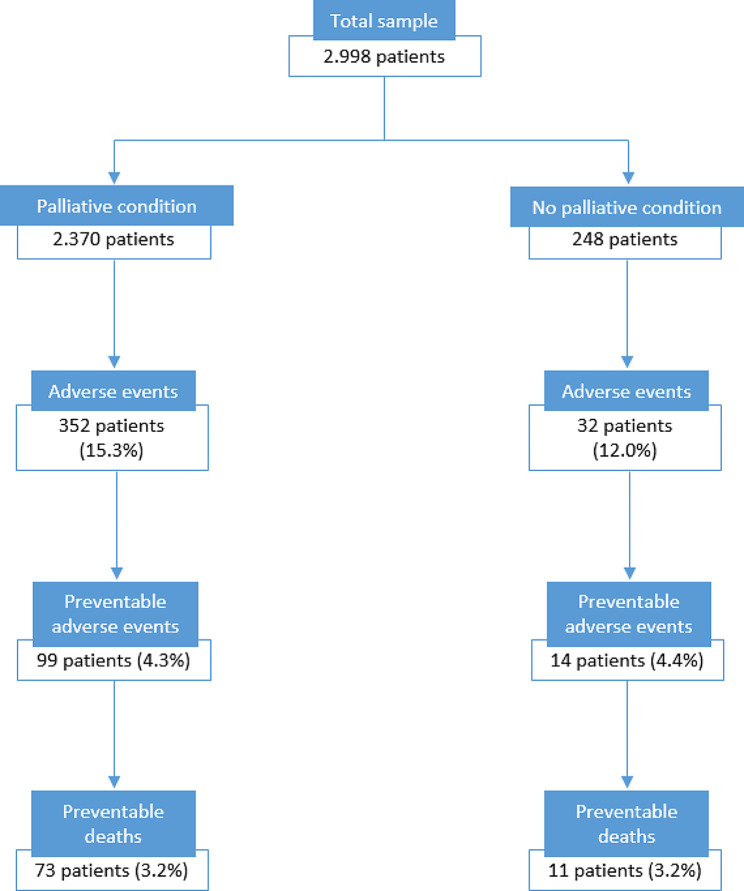
Methods: A nationwide retrospective record review study was performed in 20 Dutch hospitals. A total of 2,998 records of patients who died in hospital in 2019 was included. Records were reviewed for AEs. We identified two subgroups: patients with (n = 2,370) or without (n = 248) a condition relevant for palliative care through the selection method of Etkind (2017). Descriptive analyses were performed to calculate prevalence, nature, causes and prevention strategies. T-tests were performed to calculate differences between subgroups.
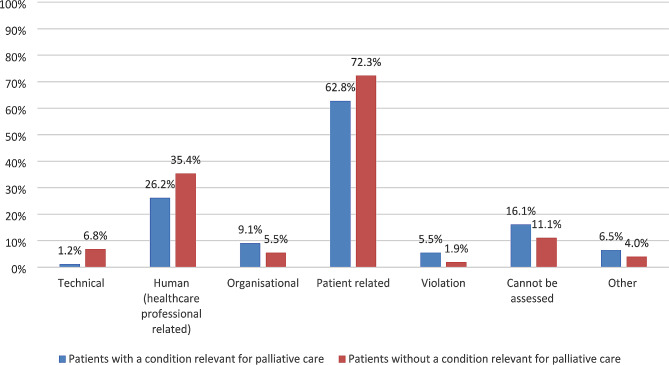
Results: We found no significant differences between subgroups regarding AE prevalence, this was 15.3% in patients with a condition relevant for palliative care, versus 12.0% in patients without a condition relevant for palliative care (p = 0.148). Potentially preventable AE prevalence was 4.3% versus 4.4% (p = 0.975). Potentially preventable death prevalence in both groups was 3.2% (p = 0.938). There were differences in the nature of AEs: in patients with a condition relevant for palliative care this was mostly related to medication (33.1%), and in patients without a condition relevant for palliative care to surgery (50.8%). In both subgroups in the majority of AEs a patient related cause was identified. For the potentially preventable AEs in both subgroups the two most important prevention strategies as suggested by the medical reviewers were reflection and evaluation and quality assurance.
Discussion: Patient safety risks appeared to be equally prevalent in both subgroups. The nature of AEs does differ between subgroups: medication- versus surgery-related, indicating that tailored safety measures are needed. Recommendations for practice are to focus on reflecting on AEs, complemented with case evaluations.
Keywords: Adverse events; End-of-life; Hospitals; Medical errors; Palliative care; Patient safety.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Adverse events and potentially preventable deaths in Dutch hospitals: results of a retrospective patient record review study.Qual Saf Health Care. 2009 Aug;18(4):297-302. doi: 10.1136/qshc.2007.025924. Qual Saf Health Care. 2009. PMID: 19651935
-
Examining Causes and Prevention Strategies of Adverse Events in Deceased Hospital Patients: A Retrospective Patient Record Review Study in the Netherlands.J Patient Saf. 2021 Jun 1;17(4):282-289. doi: 10.1097/PTS.0000000000000586. J Patient Saf. 2021. PMID: 30896559
-
The occurrence of adverse events in low-risk non-survivors in pediatric intensive care patients: an exploratory study.Eur J Pediatr. 2018 Sep;177(9):1351-1358. doi: 10.1007/s00431-018-3194-y. Epub 2018 Jun 26. Eur J Pediatr. 2018. PMID: 29946855 Free PMC article.
-
The occurrence, types, consequences and preventability of in-hospital adverse events - a scoping review.BMC Health Serv Res. 2018 Jul 4;18(1):521. doi: 10.1186/s12913-018-3335-z. BMC Health Serv Res. 2018. PMID: 29973258 Free PMC article.
-
Validation of triggers and development of a pediatric trigger tool to identify adverse events.BMC Health Serv Res. 2014 Dec 21;14:655. doi: 10.1186/s12913-014-0655-5. BMC Health Serv Res. 2014. PMID: 25527905 Free PMC article. Review.
References
-
- Schoten LvE S, Schouten B, Baartmans M, de Bruijne M, de Jong L, Waals M, Asscheman H. C. Wagner Monitor Zorggerelateerde Schade 2019: dossieronderzoek bij overleden patiënten in Nederlandse Ziekenhuizen. Nivel; 2022.
-
- van Schoten S, Eikenhorst L, van Baartmans SB, de Bruijne M, de Jong M, et al. Monitor Zorggerelateerde Schade 2019: dossieronderzoek bij overleden patiënten in Nederlandse ziekenhuizen [Adverse events monitor 2019: retrospective patient record review study of decedents in Dutch hospitals] Utrecht: Nivel; 2022.
-
- Fransen H, Dermois M, van Esch T, Oldenmenger W, Onwuteaka-Philipsen B, Raijmakers N. Kerncijfers palliatieve zorg. Utrecht: PZNL; 2019.
-
- Oosterveld-Vlug MG, Heins MJ, Boddaert MS, Engels Y, Heide Avd, Onwuteaka-Philipsen BD, et al. Evaluating quality of care at the end of life and setting best practice performance standards: a population-based observational study using linked routinely collected administrative databases. BMC Palliat Care. 2022;21(1):1–9. doi: 10.1186/s12904-022-00927-2. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
