

Retention strategies are routinely communicated to potential trial participants but often differ from what was planned in the trial protocol: an analysis of adult participant information leaflets and their corresponding protocols
- PMID: 38858790
- PMCID: PMC11163762
- DOI: 10.1186/s13063-024-08194-7
Retention strategies are routinely communicated to potential trial participants but often differ from what was planned in the trial protocol: an analysis of adult participant information leaflets and their corresponding protocols
Abstract
Background: Retaining participants in randomised controlled trials (RCTs) is challenging and trial teams are often required to use strategies to ensure retention or improve it. Other than monetary incentives, there is no requirement to disclose the use of retention strategies to the participant. Additionally, not all retention strategies are developed at the planning stage, i.e. post-funding during protocol development, but some protocols include strategies for participant retention as retention is considered and planned for early in the trial planning stage. It is yet unknown if these plans are communicated in the corresponding participant information leaflets (PILs). The purpose of our study was to determine if PILs communicate plans to promote participant retention and, if so, are these outlined in the corresponding trial protocol.
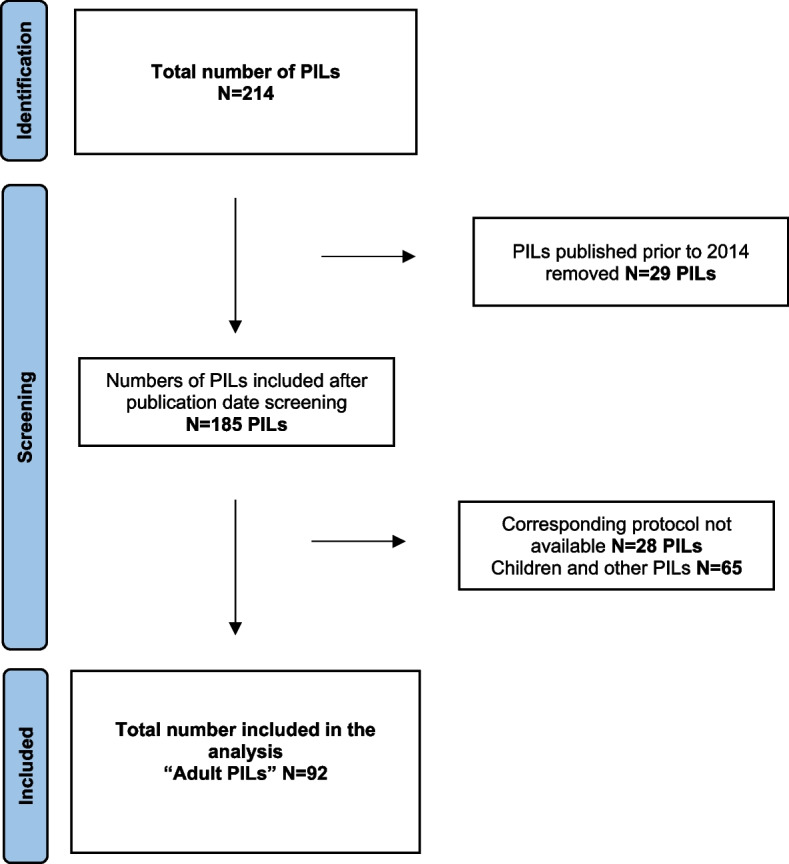
Methods: Ninety-two adult PILs and their 90 corresponding protocols from Clinical Trial Units (CTUs) in the UK were analysed. Directed (deductive) content analysis was used to analyse the participant retention text from the PILs. Data were presented using a narrative summary and frequencies where appropriate.
Results: Plans to promote participant retention were communicated in 81.5% (n = 75/92) of PILs. Fifty-seven percent (n = 43/75) of PILs communicated plans to use "combined strategies" to promote participant retention. The most common individual retention strategy was telling the participants that data collection for the trial would be scheduled during routine care visits (16%; n = 12/75 PILs). The importance of retention and the impact that missing or deleted data (deleting data collected prior to withdrawal) has on the ability to answer the research question were explained in 6.5% (n = 6/92) and 5.4% (n = 5/92) of PILs respectively. Out of the 59 PILs and 58 matching protocols that both communicated plans to use strategies to promote participant retention, 18.6% (n = 11/59) communicated the same information, the remaining 81.4% (n = 48/59) of PILs either only partially communicated (45.8%; n = 27/59) the same information or did not communicate the same information (35.6%; n = 21/59) as the protocol with regard to the retention strategy(ies).
Conclusion: Retention strategies are frequently communicated to potential trial participants in PILs; however, the information provided often differs from the content in the corresponding protocol. Participant retention considerations are best done at the planning stage of the trial and we encourage trial teams to be consistent in the communication of these strategies in both the protocol and PIL.
Keywords: Communication; Informed consent; Participant information leaflet; Patient information leaflet; Reporting; Retention; Retention strategy.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Patient information leaflets (PILs) for UK randomised controlled trials: a feasibility study exploring whether they contain information to support decision making about trial participation.Trials. 2014 Feb 18;15:62. doi: 10.1186/1745-6215-15-62. Trials. 2014. PMID: 24548781 Free PMC article.
-
When describing harms and benefits to potential trial participants, participant information leaflets are inadequate.Trials. 2024 May 1;25(1):292. doi: 10.1186/s13063-024-08087-9. Trials. 2024. PMID: 38693579 Free PMC article.
-
Relative importance of informational items in participant information leaflets for trials: a Q-methodology approach.BMJ Open. 2018 Sep 5;8(9):e023303. doi: 10.1136/bmjopen-2018-023303. BMJ Open. 2018. PMID: 30185580 Free PMC article.
-
How do trial teams plan for retention during the design stage of the trial? A scoping review.Trials. 2023 Dec 4;24(1):784. doi: 10.1186/s13063-023-07775-2. Trials. 2023. PMID: 38049833 Free PMC article.
-
Recommendations for developing accessible patient information leaflets for clinical trials to address English language literacy as a barrier to research participation.Trials. 2024 Sep 27;25(1):624. doi: 10.1186/s13063-024-08471-5. Trials. 2024. PMID: 39334243 Free PMC article. Review.
Cited by
-
Evaluating the use of SPIRIT on participant retention in randomised trials: Challenges in reporting and implications for practice.PLoS One. 2025 Aug 12;20(8):e0327110. doi: 10.1371/journal.pone.0327110. eCollection 2025. PLoS One. 2025. PMID: 40794667 Free PMC article.
References
-
- Brunsdon D, Biesty L, Brocklehurst P, Brueton V, Devane D, Elliott J, et al. What are the most important unanswered research questions in trial retention? A James Lind Alliance Priority Setting Partnership: the PRioRiTy II (Prioritising Retention in Randomised Trials) study. Trials. 2019;20(1):1–12. doi: 10.1186/s13063-019-3687-7. - DOI - PMC - PubMed
-
- Walters SJ, dos Anjos Henriques-Cadby IB, Bortolami O, Flight L, Hind D, Jacques RM, et al. Recruitment and retention of participants in randomised controlled trials: a review of trials funded and published by the United Kingdom Health Technology Assessment Programme. BMJ open. 2017;7(3):e015276. doi: 10.1136/bmjopen-2016-015276. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
