

Cervical Alignment and Range of Motion Change after Anterior 3-Level Hybrid Surgery Compared with Cervical Laminoplasty: A Matched Cohort Study
- PMID: 38859705
- PMCID: PMC11293915
- DOI: 10.1111/os.14120
Cervical Alignment and Range of Motion Change after Anterior 3-Level Hybrid Surgery Compared with Cervical Laminoplasty: A Matched Cohort Study
Abstract
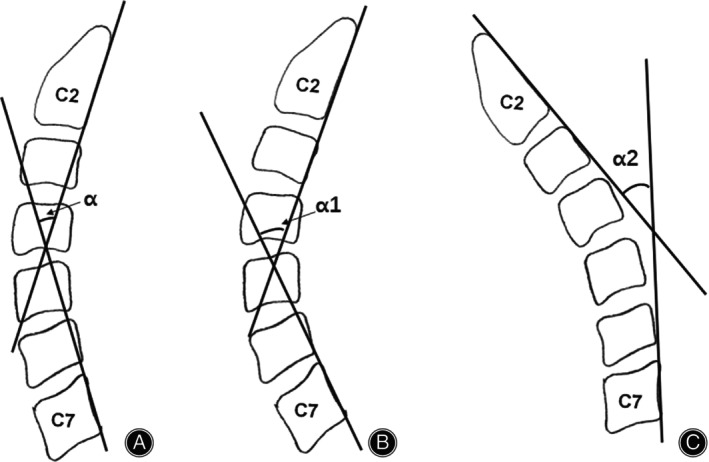
Objectives: Cervical alignment and range of motion (ROM) changes after cervical spine surgery are related to cervical biomechanical and functions. Few studies compared these parameters between posterior laminoplasty and anterior 3-level hybrid surgery incorporating anterior cervical discectomy and fusion (ACDF) with cervical disc replacement (CDR). This study is aimed to detect the differences of cervical alignment and ROM changes of the two surgeries in a matched-cohort study.
Methods: From January 2018 and May 2020, 51 patients who underwent 3-level hybrid surgery incorporating ACDF with ACDR were included. A 1:1 match of the patients who underwent cervical laminoplasty based on age, gender, duration of symptoms, body mass index, and cervical alignment type was utilized as control group. General data (operative time, blood loss, etc.), Japanese Orthopaedic Association (JOA) score, VAS (Visual Analog Score), NDI (The Neck Disability Index), cervical sagittal alignment, and cervical range of motion (ROM) were recorded and compared.
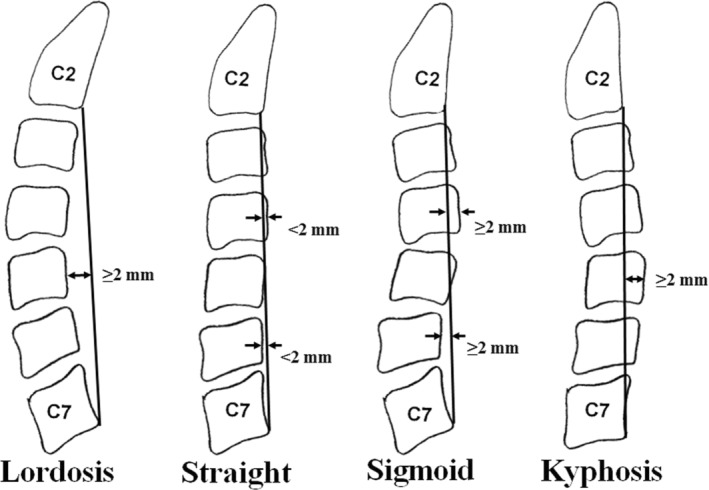
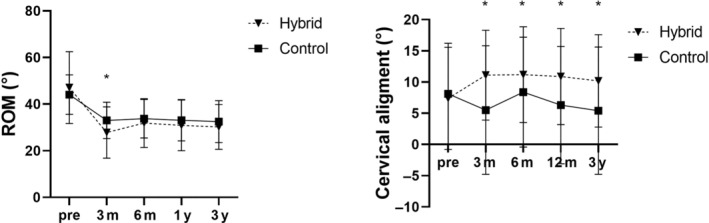
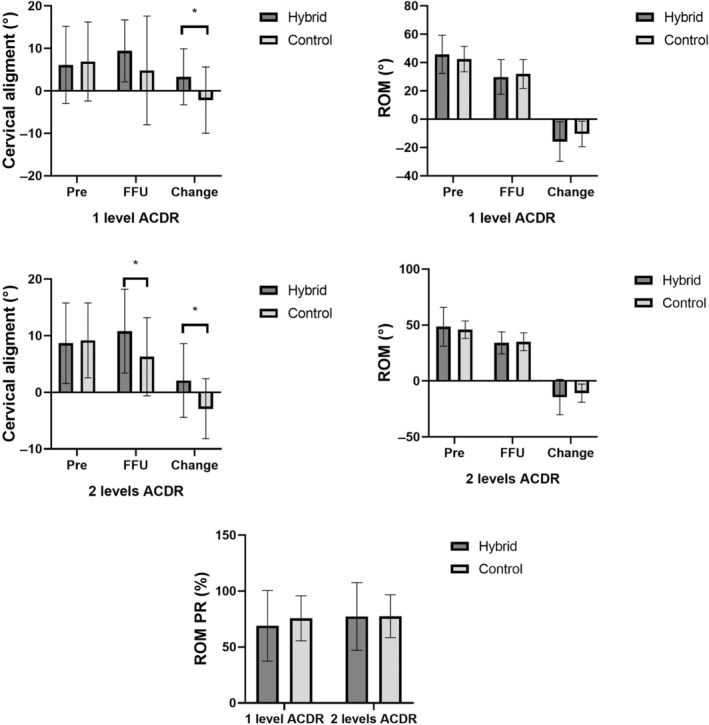
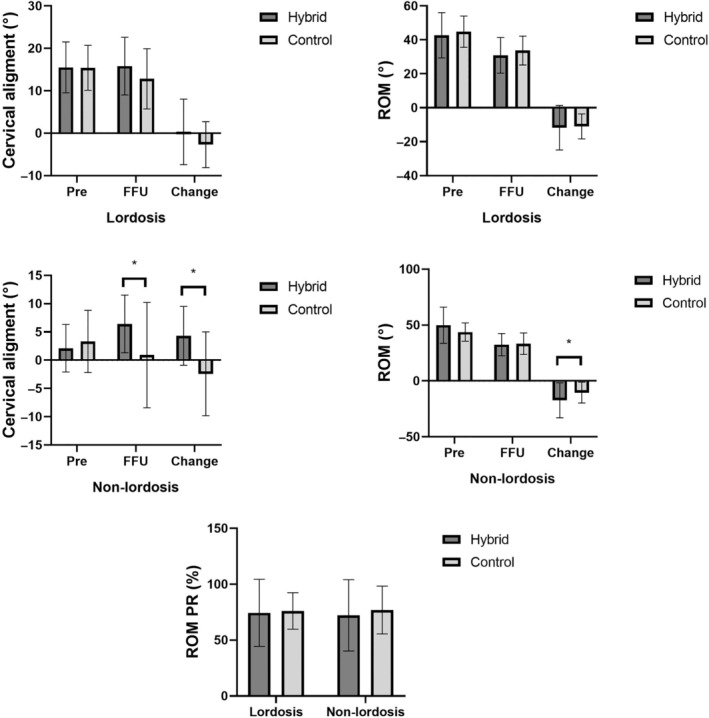
Results: Both groups gained significant improvement in JOA, VAS, NDI scores postoperatively (p < 0.05). Cervical alignment significantly increased in hybrid group and decreased in control group after surgeries (p < 0.001). ROM decrease was similar in two groups. For cervical lordosis, though cervical alignment angle in control group decreased, the final follow-up cervical alignment and cervical alignment changes were not significantly different between hybrid and control groups. For cervical non-lordosis, cervical alignment decreased in control group while increased in hybrid group. At final follow-up, cervical alignment and the changes between the two groups were significantly different. Both control group and hybrid group had similar ROM decrease after the surgery no matter whether there was cervical lordosis or non-lordosis. Hybrid surgery showed cervical alignments significantly improved and similar ROM preservation compared with control group at final follow-up both for 1-level and 2-level disc replacement subgroups.
Conclusions: The hybrid surgery demonstrated advantages of preserving cervical alignment and gaining similar cervical ROM preservation compared with cervical laminoplasty, especially for cervical non-lordosis. Given the importance of restoring lordotic cervical alignment, hybrid surgery may be preferred over laminoplasty to treat multilevel cervical disc herniation.
Keywords: Anterior Hybrid Surgery; Cervical Spine Alignment; Laminoplasty; Non‐Lordosis; ROM.
© 2024 The Author(s). Orthopaedic Surgery published by Tianjin Hospital and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare that they have no conflict of interest concerning the materials or methods used in this study or the findings specified in this study. No relevant financial activities outside the submitted work need to be declared.
Figures
References
-
- Scheer JK, Tang JA, Smith JS, Protopsaltis TS, Blondel B, Bess S, et al. Cervical spine alignment, sagittal deformity, and clinical implications: a review. J Neurosurg Spine. 2013;19(2):141–159. - PubMed
-
- Ames CP, Blondel B, Scheer JK, Schwab FJ, le Huec JC, Massicotte EM, et al. Cervical radiographical alignment: comprehensive assessment techniques and potential importance in cervical myelopathy. Spine (Phila Pa 1976). 2013;38(22 Suppl 1):S149–S160. - PubMed
-
- Tundo F, Avila MJ, Willard L, Fanous S, Curri C, Hussain I, et al. Spinal alignment, surgery, and outcomes in cervical deformity: a practical guide to aid the spine surgeon. Clin Neurol Neurosurg. 2019;185:105496. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
