

Long-term outcomes of ADEM-like and tumefactive presentations of CNS demyelination: a case-comparison analysis
- PMID: 38861035
- PMCID: PMC11319424
- DOI: 10.1007/s00415-024-12349-6
Long-term outcomes of ADEM-like and tumefactive presentations of CNS demyelination: a case-comparison analysis
Abstract
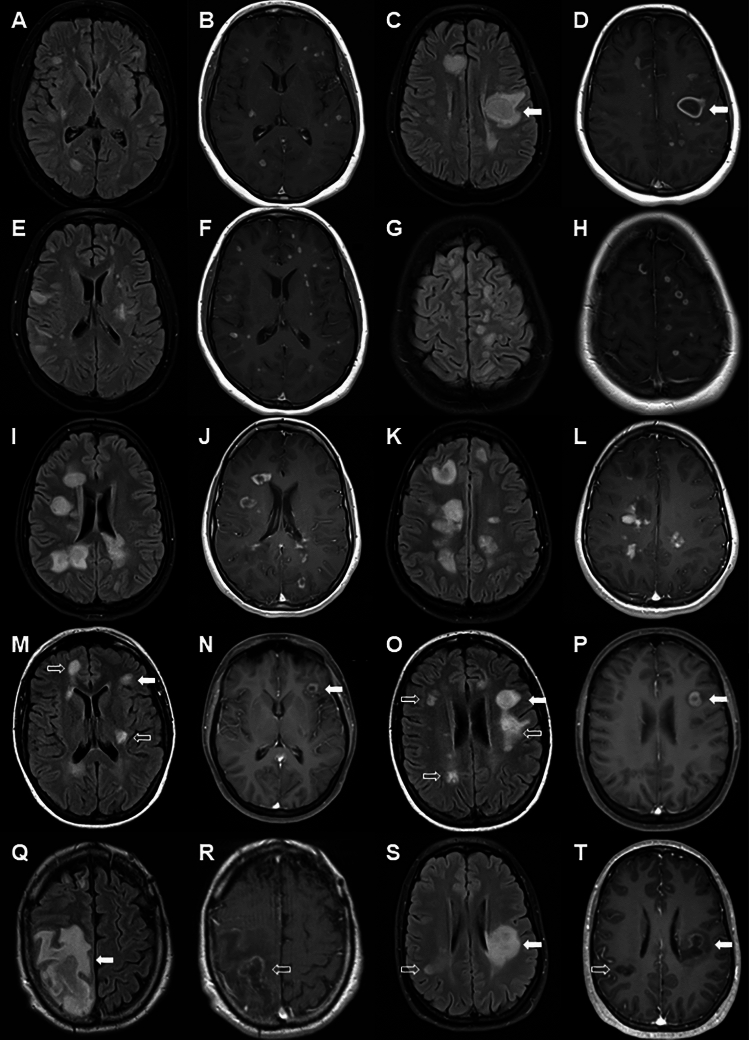
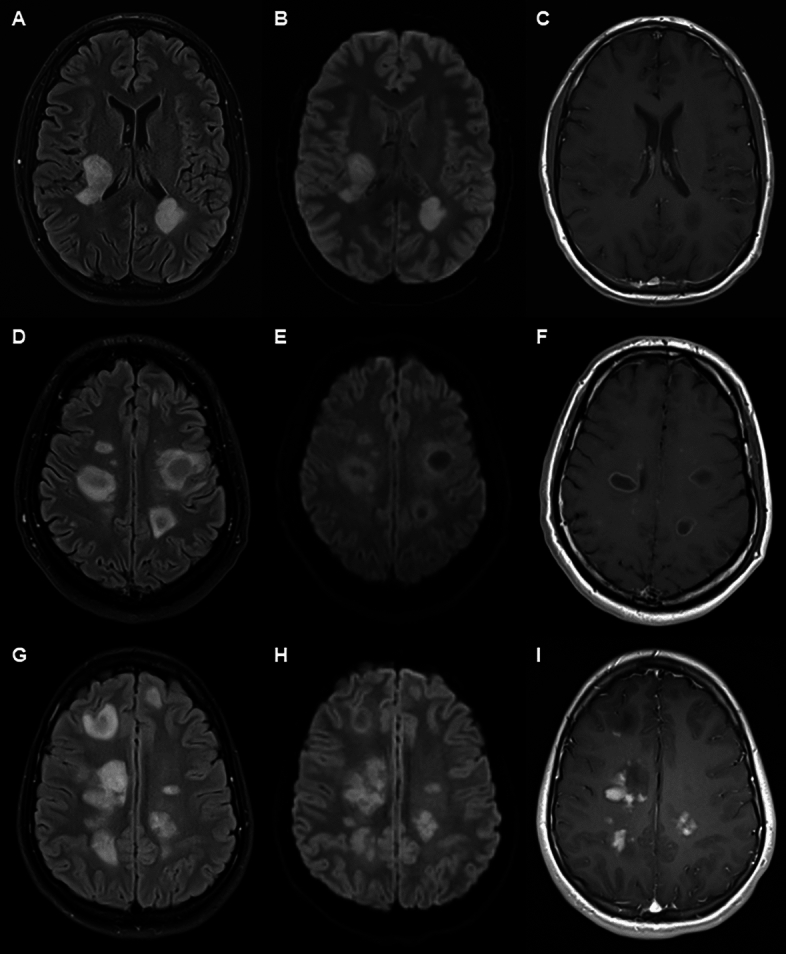
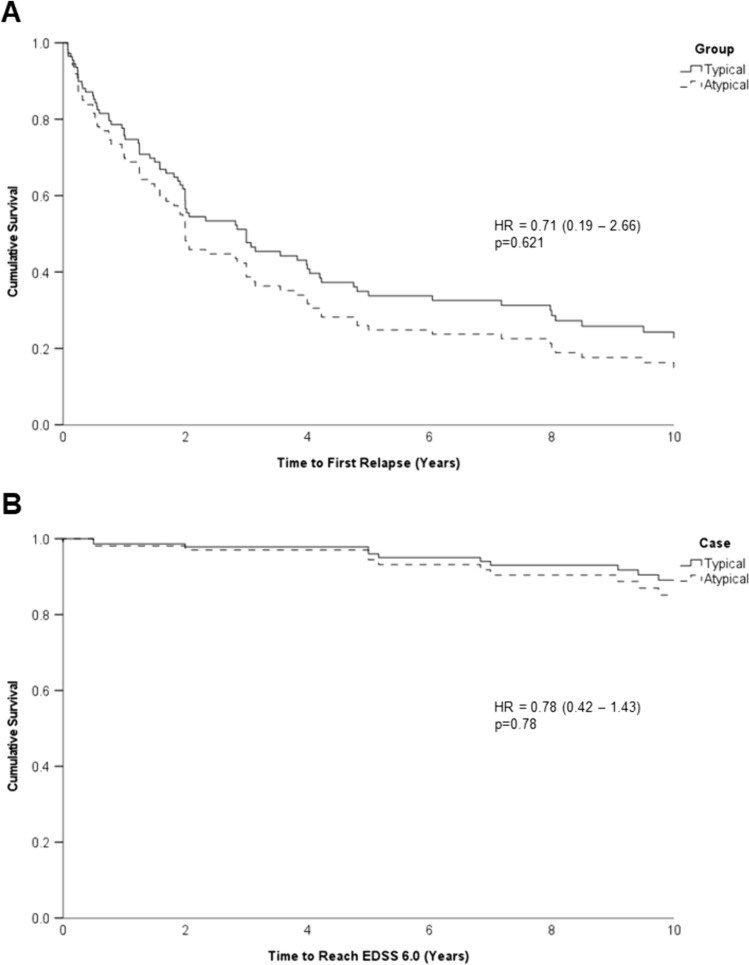
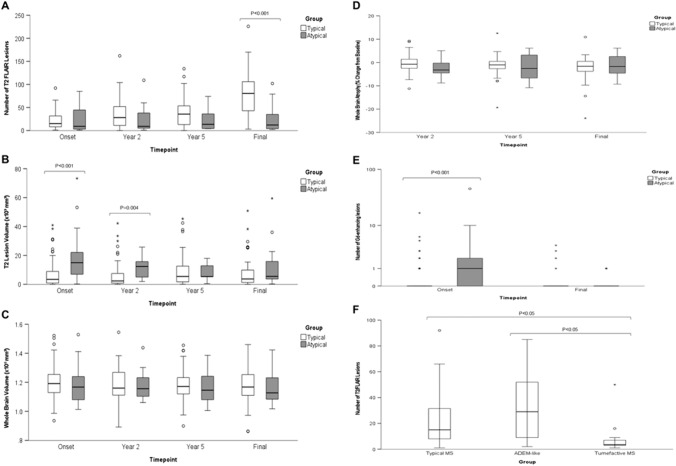
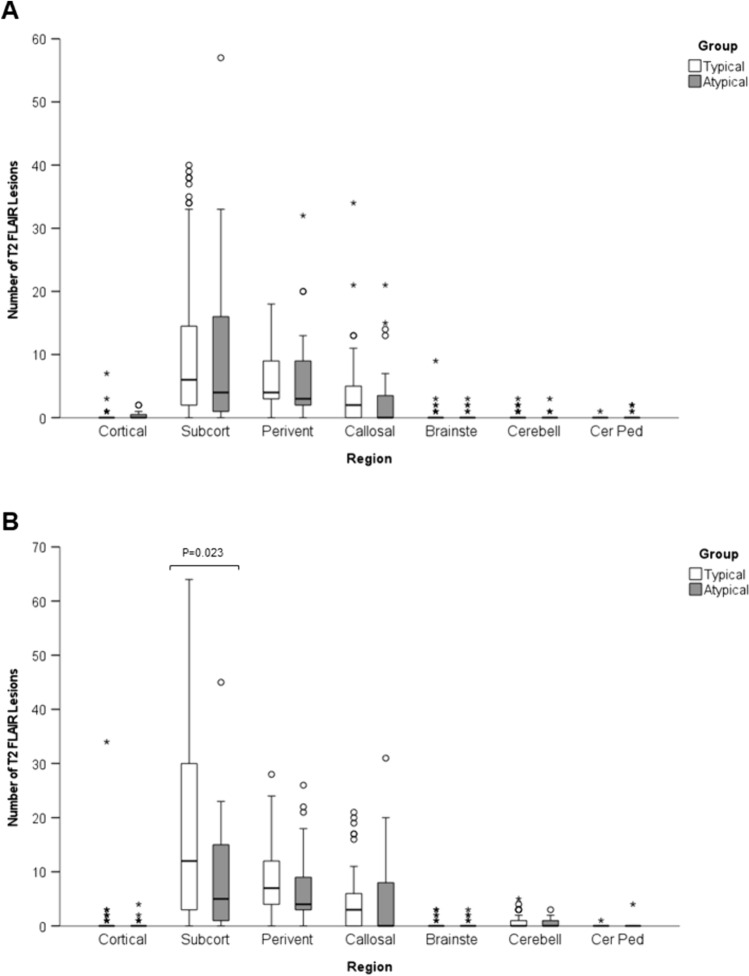
A minority of initial multiple sclerosis (MS) presentations clinically or radiologically resemble other central nervous system (CNS) pathologies, acute disseminated encephalomyelitis (ADEM) or tumefactive demyelination (atypical demyelination presentations). With the aim of better defining the long-term outcomes of this group we have performed a retrospective cohort comparison of atypical demyelination versus 'typical' MS presentations. Twenty-seven cases with atypical presentations (both first and subsequent demyelinating events) were identified and compared with typical MS cases. Disease features analysed included relapse rates, disability severity, whole brain and lesion volumes, lesion number and distribution. Atypical cases represented 3.9% of all MS cases. There was considerable overlap in the magnetic resonance imaging (MRI) features of ADEM-like and tumefactive demyelination cases. ADEM-like cases tended to be younger but not significantly so. Atypical cases showed a trend towards higher peak expanded disability severity score (EDSS) score at the time of their atypical presentation. Motor, cranial nerve, cerebellar, cerebral and multifocal presentations were all more common in atypical cases, and less likely to present with optic neuritis. Cerebrospinal fluid (CSF) white cell counts were higher in atypical cases (p = 0.002). One atypical case was associated with peripheral blood myelin oligodendrocyte glycoprotein (MOG) antibodies, but subsequent clinical and radiological course was in keeping with MS. There was no difference in long-term clinical outcomes including annualised relapse rates (ARR), brain volume, lesion numbers or lesion distributions. Atypical demyelination cases were more likely to receive high potency disease modifying therapy early in the course of their illness. Despite the severity of initial illness, our cohort analysis suggests that atypical demyelination presentations do not confer a higher risk of long-term adverse outcomes.
Keywords: Acute disseminated encephalomyelitis; Multiple sclerosis; Prognosis; Tumefactive.
© 2024. Crown.
Conflict of interest statement
SAB has received honoraria for attendance at advisory boards and travel sponsorship from Bayer-Schering, Biogen-Idec, Merck-Serono, Novartis, and Sanofi-Genzyme, has received speakers honoraria from Biogen-Idec and Genzyme, is an investigator in clinical trials sponsored by Biogen Idec, Novartis and Genzyme, and was the recipient of an unencumbered research grant from Biogen-Idec. Dr Sudarshini Ramanathan has received research funding from the National Health and Medical Research Council (Australia), the Brain Foundation (Australia), the Royal Australasian College of Physicians, the Petre Foundation, and the University of Sydney. She is supported by an NHMRC Investigator Grant (GNT2008339). She serves as a consultant on an advisory board for UCB and Limbic Neurology, and has been an invited speaker for Biogen, Excemed, and Limbic Neurology. SVA has accept financial support to attend conferences supported by Biogen. KP, SR, SB, FB report no relevant financial disclosures.
Figures
Similar articles
-
Acute disseminated encephalomyelitis, multiphasic disseminated encephalomyelitis and multiple sclerosis in children.Brain. 2000 Dec;123 Pt 12:2407-22. doi: 10.1093/brain/123.12.2407. Brain. 2000. PMID: 11099444 Clinical Trial.
-
Clinical course, therapeutic responses and outcomes in relapsing MOG antibody-associated demyelination.J Neurol Neurosurg Psychiatry. 2018 Feb;89(2):127-137. doi: 10.1136/jnnp-2017-316880. Epub 2017 Nov 15. J Neurol Neurosurg Psychiatry. 2018. PMID: 29142145 Free PMC article.
-
Perivenous demyelination: association with clinically defined acute disseminated encephalomyelitis and comparison with pathologically confirmed multiple sclerosis.Brain. 2010 Feb;133(Pt 2):333-48. doi: 10.1093/brain/awp321. Epub 2010 Feb 3. Brain. 2010. PMID: 20129932 Free PMC article.
-
Exploring the overlap between multiple sclerosis, tumefactive demyelination and Baló's concentric sclerosis.Mult Scler. 2016 Jul;22(8):986-92. doi: 10.1177/1352458516641776. Epub 2016 Apr 1. Mult Scler. 2016. PMID: 27037180 Review.
-
Atypical Pediatric Demyelinating Diseases of the Central Nervous System.Curr Neurol Neurosci Rep. 2019 Nov 26;19(12):95. doi: 10.1007/s11910-019-1015-y. Curr Neurol Neurosci Rep. 2019. PMID: 31773416 Review.
Cited by
-
Clinical Spectrum of Acquired Demyelinating Syndromes in Children: A Tertiary Hospital Experience.Neurol Ther. 2025 Aug;14(4):1495-1506. doi: 10.1007/s40120-025-00768-0. Epub 2025 Jun 4. Neurol Ther. 2025. PMID: 40461933 Free PMC article.
References
-
- McDonald WI, Compston A, Edan G, Goodkin D, Hartung HP, Lublin FD, McFarland HF, Paty DW, Polman CH, Reingold SC, Sandberg-Wollheim M, Sibley W, Thompson A, van den Noort S, Weinshenker BY, Wolinsky JS (2001) Recommended diagnostic criteria for multiple sclerosis: guidelines from the international panel on the diagnosis of multiple sclerosis. Ann Neurol 50:121–127 10.1002/ana.1032 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
