

Laparoscopic left hepatectomy for a patient with an absence of portal bifurcation using real-time imaging: a case report
- PMID: 38861107
- PMCID: PMC11166617
- DOI: 10.1186/s40792-024-01945-3
Laparoscopic left hepatectomy for a patient with an absence of portal bifurcation using real-time imaging: a case report
Abstract
Background: Absence of portal bifurcation is an extremely rare anomaly that should be recognized preoperatively, especially prior to a major hepatectomy.
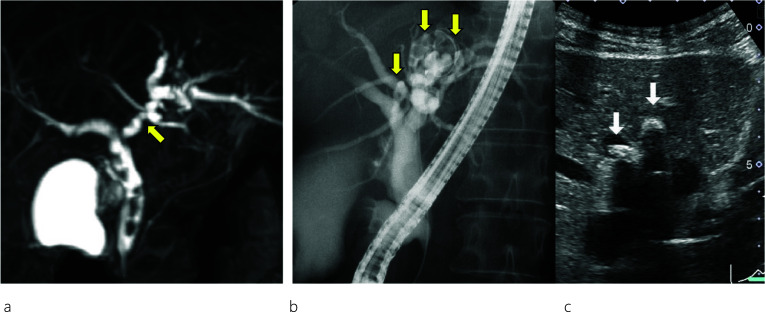
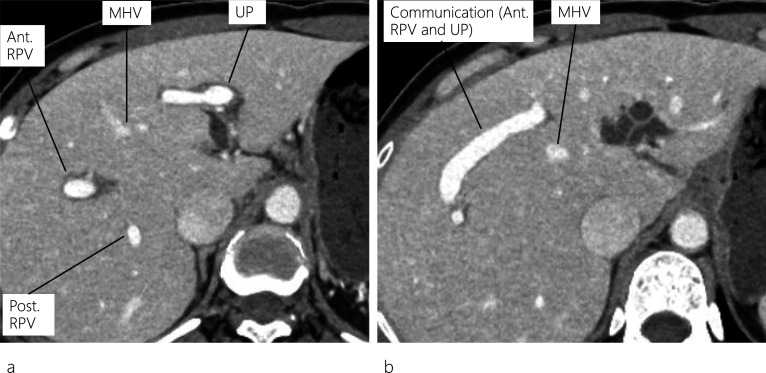
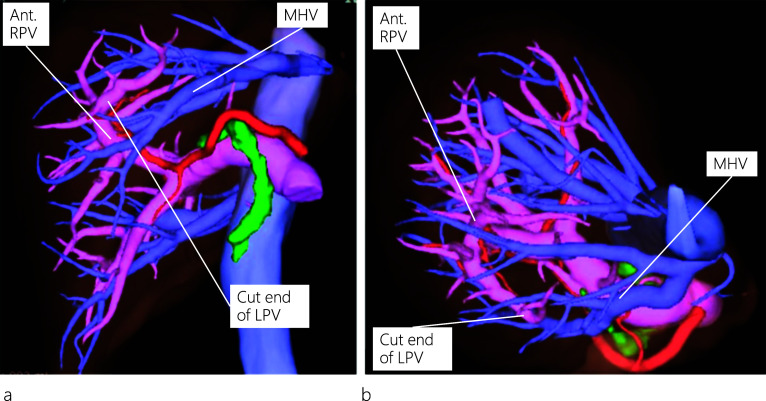
Case presentation: A 45-year-old woman presented with abdominal pain, and abdominal computed tomography (CT) revealed dilatation of both the common bile duct (CBD) and intrahepatic bile duct (IHBD). Endoscopic retrograde cholangiopancreatography (ERCP) showed CBD and IHBD stones (B2 and B4). The CBD stones were removed, but the IHBD stones could not be, yet there was no evidence of malignancy at the site of IHBD stenosis. Enhanced CT revealed a dilated IHBD, while three-dimensional CT images showed the left portal vein running through the ventral side of the middle hepatic vein, which was diagnosed as the absence of portal vein bifurcation (APB). Laparoscopic left hepatectomy was successfully performed using real-time indocyanine green (ICG) fluorescence imaging.
Conclusion: Surgeons should be aware of the possibility of APB, a rare portal vein anomaly, before performing major hepatectomy. Real-time ICG fluorescence imaging may be helpful to ensure the precise anatomy of the liver during laparoscopic surgery.
Keywords: Absence of portal vein bifurcation; ICG fluorescence real-time imaging; Laparoscopic left hepatectomy; Portal vein anomaly.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests associated with this manuscript.
Figures


References
LinkOut - more resources
Full Text Sources
