

Defining the optimal target-to-background ratio to identify positive lymph nodes in prostate cancer patients undergoing robot-assisted [99mTc]Tc-PSMA radioguided surgery: updated results and ad interim analyses of a prospective phase II study
- PMID: 38861182
- PMCID: PMC11445289
- DOI: 10.1007/s00259-024-06789-5
Defining the optimal target-to-background ratio to identify positive lymph nodes in prostate cancer patients undergoing robot-assisted [99mTc]Tc-PSMA radioguided surgery: updated results and ad interim analyses of a prospective phase II study
Abstract
Introduction: Prostate-specific membrane antigen radioguided surgery (PSMA-RGS) might identify lymph node invasion (LNI) in prostate cancer (PCa) patients undergoing extended pelvic lymph node dissection (ePLND). The optimal target-to-background (TtB) ratio to define RGS positivity is still unknown.
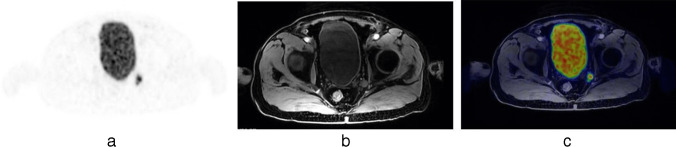
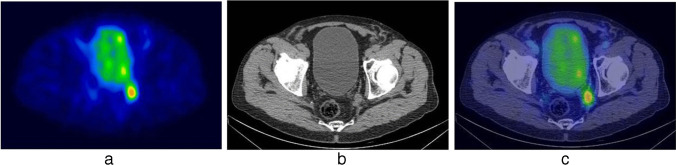
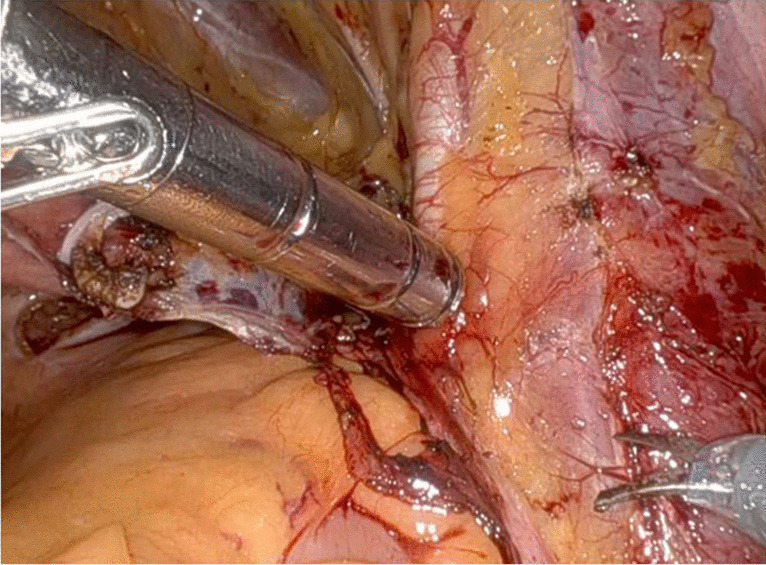
Materials & methods: Ad interim analyses which focused on 30 patients with available pathological information were conducted. All patients underwent preoperative PSMA positron emission tomography (PET). 99m-Technetium-PSMA imaging and surgery ([99mTc]Tc-PSMA-I&S) was administered the day before surgery. In vivo measurements were conducted using an intraoperative gamma probe. Performance characteristics and implications associated with different TtB ratios were assessed.
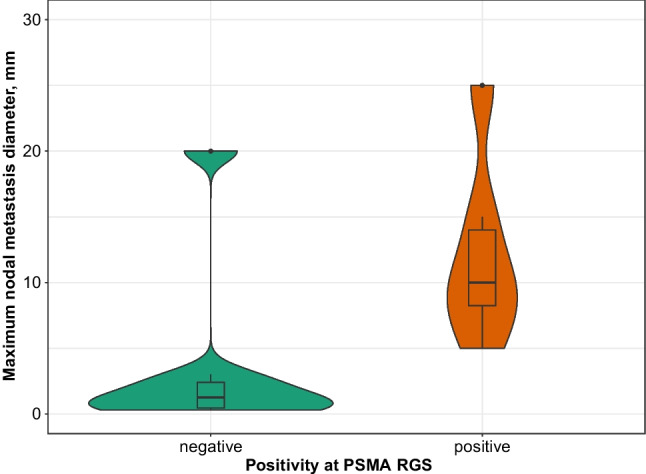
Results: Overall, 9 (30%) patients had LNI, with 22 (13%) and 80 (11%) positive regions and lymph nodes, respectively. PSMA-RGS showed uptakes in 12 (40%) vs. 7 (23%) vs. 6 (20%) patients for a TtB ratio ≥ 2 vs. ≥ 3 vs. ≥ 4. At a per-region level, sensitivity, specificity and accuracy for a TtB ratio ≥ 2 vs. ≥ 3 vs. ≥ 4 were 72%, 88% and 87% vs. 54%, 98% and 92% vs. 36%, 99% and 91%. Performing ePLND only in patients with suspicious spots at PSMA PET (n = 7) would have spared 77% ePLNDs at the cost of missing 13% (n = 3) pN1 patients. A TtB ratio ≥ 2 at RGS identified 8 (24%) suspicious areas not detected by PSMA PET, of these 5 (63%) harbored LNI, with one pN1 patient (11%) that would have been missed by PSMA PET. Adoption of a TtB ratio ≥ 2 vs. ≥ 3 vs. ≥ 4, would have allowed to spare 18 (60%) vs. 23 (77%) vs. 24 (80%) ePLNDs missing 2 (11%) vs. 3 (13%) vs. 4 (17%) pN1 patients.
Conclusions: PSMA-RGS using a TtB ratio ≥ 2 to identify suspicious nodes, could allow to spare > 50% ePLNDs and would identify additional pN1 patients compared to PSMA PET and higher TtB ratios.
Keywords: Lymph node dissection; Lymph node metastases; Prostate cancer; Prostate-specific membrane antigen; Radioguided surgery; Staging.
© 2024. The Author(s).
Conflict of interest statement
Financial interests: Alberto Briganti and Arturo Chiti declared their conflict of interest.
Alberto Briganti declared the following conflict of interest:
• Astellas Pharma Janseen-Cilag
• OPKO Health
• MDx Health
• Bayer
• miR Scientific
• LLC (“miR”)
• A3P biomedical
• MSD/Astrazeneca
• Ferring
• Pfizer
• Sandoz-Novartis
• Telix Pharmaceuticals
• European Urology, Editor in Chief
Arturo Chiti declared the following conflict of interest:
• Novartis, advisory board; speaker honorarium
• AAA, advisory board; speaker honorarium
• Sirtex, speaker honorarium
• General Electric Healthcare, speaker’s honorarium
• Telix, advisory board
• Bracco, speaker honorarium
• European Journal of Nuclear Medicine and Molecular Imaging, Editor in Chief
Figures
References
-
- Maurer T, et al. Prostate-specific membrane antigen-radioguided surgery for metastatic lymph nodes in prostate cancer. Eur Urol. 2015;68(3). 10.1016/j.eururo.2015.04.034. - PubMed
-
- Barletta F, et al. The role of nuclear medicine tracers for prostate cancer surgery: from preoperative to intraoperative setting. Curr Opin Urol. 2023;33(6):502–9. 10.1097/MOU.0000000000001118. (Lippincott Williams and Wilkins). - PubMed
-
- Gandaglia G, et al. Prostate-specific membrane antigen radioguided surgery to detect nodal metastases in primary prostate cancer patients undergoing robot-assisted radical prostatectomy and extended pelvic lymph node dissection: results of a planned interim analysis of a prospective phase 2 study. Eur Urol. 2022;82(4):411–8. 10.1016/j.eururo.2022.06.002. - PubMed
-
- Maurer T, et al. 99m Technetium-based prostate-specific membrane antigen–radioguided surgery in recurrent prostate cancer. Eur Urol. 2019;75(4):659–66. 10.1016/j.eururo.2018.03.013. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
