

Data-Driven Phenotyping of Presymptomatic Type 1 Diabetes Using Longitudinal Autoantibody Profiles
- PMID: 38861550
- PMCID: PMC11272969
- DOI: 10.2337/dc24-0198
Data-Driven Phenotyping of Presymptomatic Type 1 Diabetes Using Longitudinal Autoantibody Profiles
Abstract
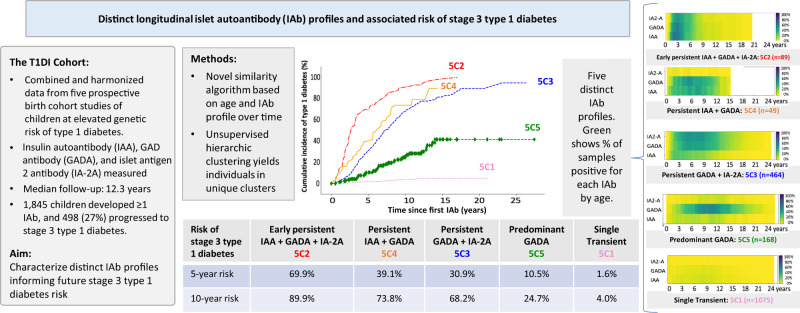
Objective: To characterize distinct islet autoantibody profiles preceding stage 3 type 1 diabetes.
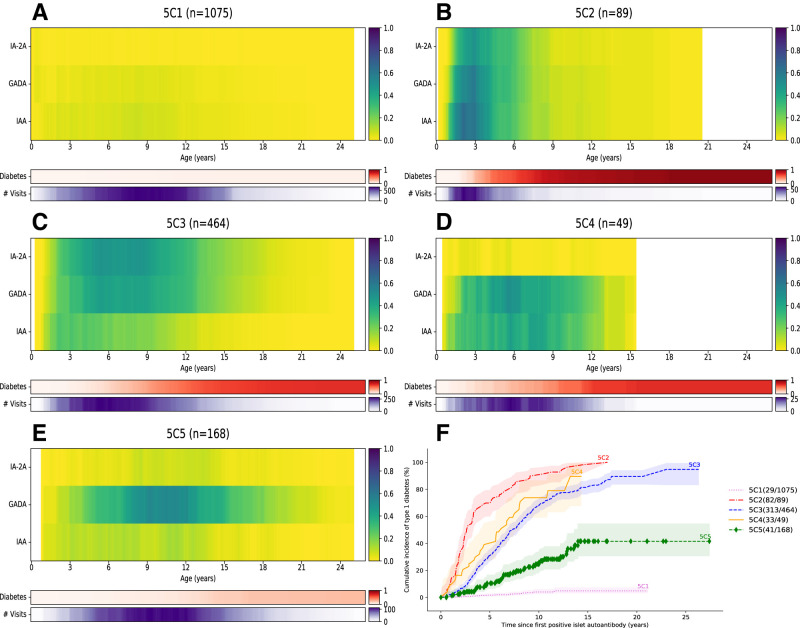
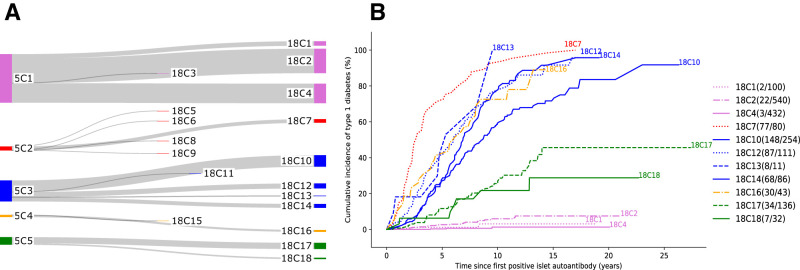
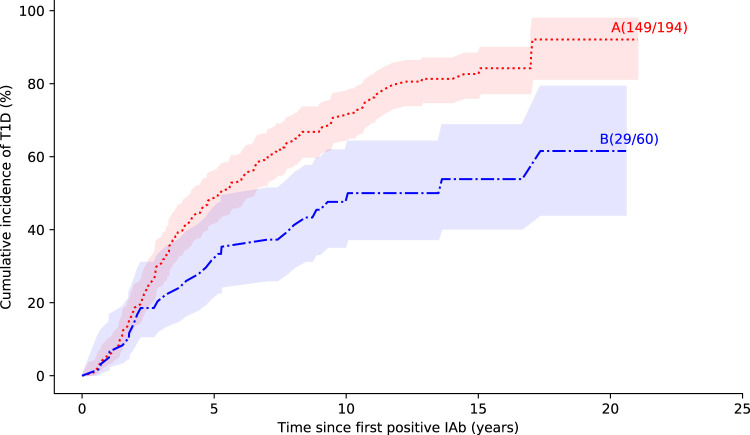
Research design and methods: The T1DI (Type 1 Diabetes Intelligence) study combined data from 1,845 genetically susceptible prospectively observed children who were positive for at least one islet autoantibody: insulin autoantibody (IAA), GAD antibody (GADA), or islet antigen 2 antibody (IA-2A). Using a novel similarity algorithm that considers an individual's temporal autoantibody profile, age at autoantibody appearance, and variation in the positivity of autoantibody types, we performed an unsupervised hierarchical clustering analysis. Progression rates to diabetes were analyzed via survival analysis.
Results: We identified five main clusters of individuals with distinct autoantibody profiles characterized by seroconversion age and sequence of appearance of the three autoantibodies. The highest 5-year risk from first positive autoantibody to type 1 diabetes (69.9%; 95% CI 60.0-79.2) was observed in children who first developed IAA in early life (median age 1.6 years) followed by GADA (1.9 years) and then IA-2A (2.1 years). Their 10-year risk was 89.9% (95% CI 81.9-95.4). A high 5-year risk was also found in children with persistent IAA and GADA (39.1%) and children with persistent GADA and IA-2A (30.9%). A lower 5-year risk (10.5%) was observed in children with a late appearance of persistent GADA (6.1 years). The lowest 5-year diabetes risk (1.6%) was associated with positivity for a single, often reverting, autoantibody.
Conclusions: The novel clustering algorithm identified children with distinct islet autoantibody profiles and progression rates to diabetes. These results are useful for prediction, selection of individuals for prevention trials, and studies investigating various pathways to type 1 diabetes.
© 2024 by the American Diabetes Association.
Conflict of interest statement
Figures
References
-
- Gorus FK, Balti EV, Messaaoui A, et al. .; Belgian Diabetes Registry . Twenty-year progression rate to clinical onset according to autoantibody profile, age, and HLA-DQ genotype in a registry-based group of children and adults with a first-degree relative with type 1 diabetes. Diabetes Care 2017;40:1065–1072 - PubMed
-
- Bauer W, Veijola R, Lempainen J, et al. . Age at seroconversion, HLA genotype, and specificity of autoantibodies in progression of islet autoimmunity in childhood. J Clin Endocrinol Metab 2019;104:4521–4530 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
