

Investigating age and ethnicity as novel high-risk phenotypes in mucinous ovarian cancer: retrospective study in a multi-ethnic population
- PMID: 38862154
- PMCID: PMC11420762
- DOI: 10.1136/ijgc-2024-005332
Investigating age and ethnicity as novel high-risk phenotypes in mucinous ovarian cancer: retrospective study in a multi-ethnic population
Abstract
Objectives: Primary mucinous ovarian carcinoma represents 3% of ovarian cancers and is typically diagnosed early, yielding favorable outcomes. This study aims to identify risk factors, focussing on the impact of age and ethnicity on survival from primary mucinous ovarian cancer.
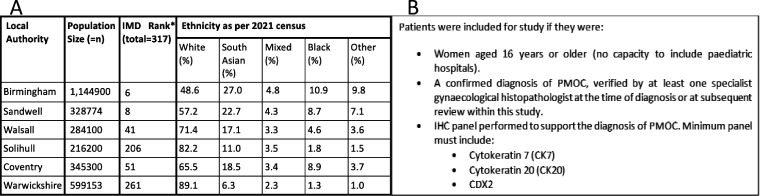
Methods: A retrospective observational study of patients treated at Sandwell and West Birmingham Hospitals NHS Trust and University Hospital Coventry and Warwickshire. Patients included were women aged ≥16 years, with primary mucinous ovarian cancer confirmed by specialist gynecological histopathologist and tumor immunohistochemistry, including cytokeratin-7, cytokeratin-20, and CDX2. Statistical analyses were performed using R integrated development environment, with survival assessed by Cox proportional hazards models and Kaplan-Meier plots.
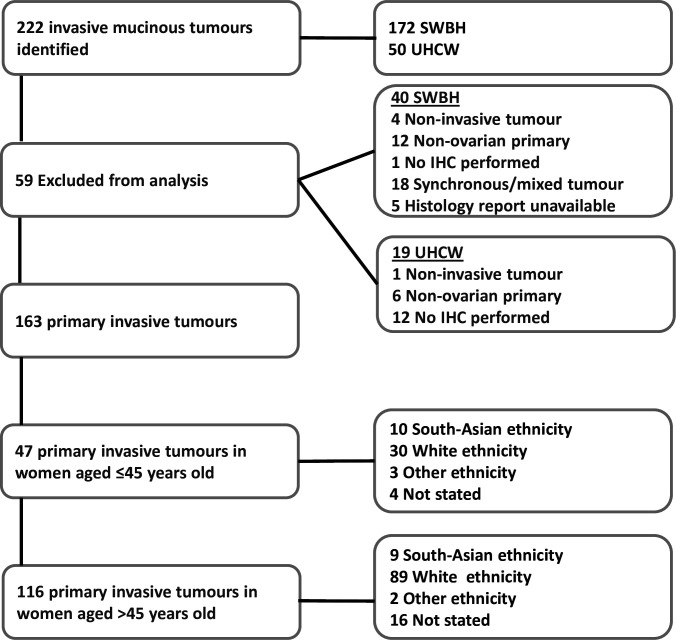
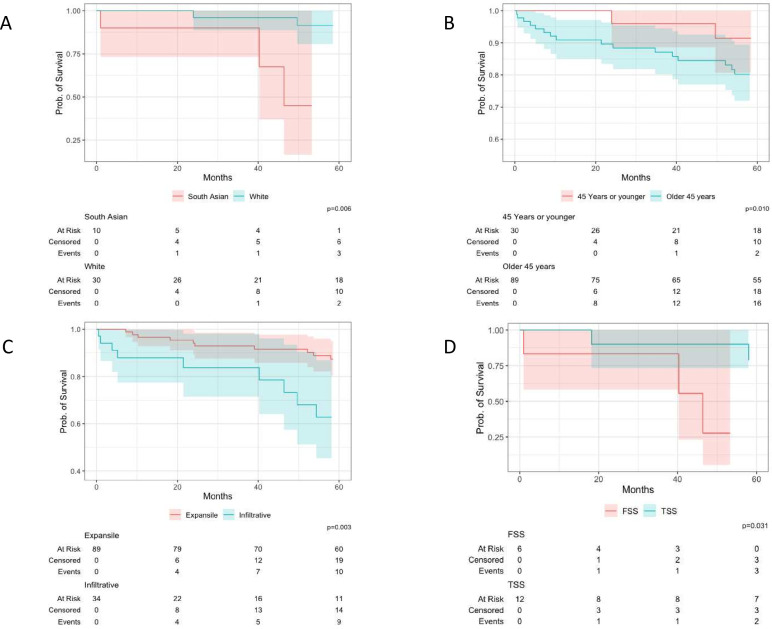
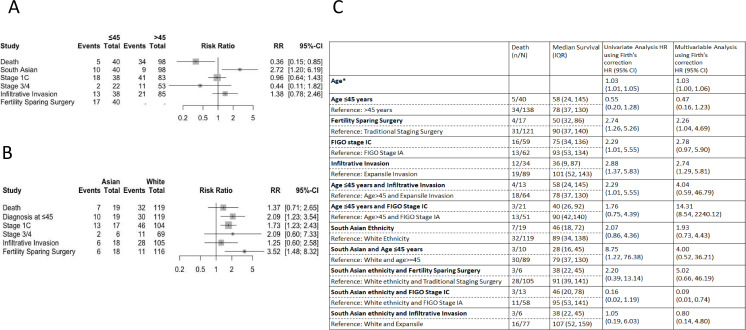
Results: A total of 163 patients were analyzed; median age at diagnosis was 58 years (range 16-92), 145 (89%) were International Federation of Gynecology and Obstetrics stage I and 43 (26%) patients had infiltrative invasion. Women aged ≤45 years were more likely to have infiltrative invasion (RR=1.38, 95% CI 0.78 to 2.46), with increased risk of death associated with infiltrative invasion (HR=2.29, 95% CI 1.37 to 5.83). Compared with White counterparts, South Asian women were more likely to undergo fertility-sparing surgery (RR=3.52, 95% CI 1.48 to 8.32), and have infiltrative invasion (RR=1.25, 95% CI 0.60 to 2.58). South Asian women undergoing fertility-sparing surgery had worse prognosis than those undergoing traditional staging surgery (HR=2.20, 95% CI 0.39 to 13.14). In FIGO stage I disease, 59% South Asian and 37% White women received adjuvant chemotherapy (p=0.06). South Asian women exhibited a worse overall prognosis than White women (HR=2.07, 95% CI 0.86 to 4.36), particularly pronounced in those aged ≤45 years (HR=8.75, 95% CI 1.22 to 76.38).
Conclusion: This study identified young age as a risk factor for diagnosis of infiltrative invasion. Fertility-sparing surgery in South Asian women is a risk factor for poorer prognosis. South Asian women exhibit poorer overall survival than their White counterparts.
Keywords: Cystadenocarcinoma, Mucinous; Ovarian Cancer; Pathology; Surgery.
© IGCS and ESGO 2024. Re-use permitted under CC BY-NC. No commercial re-use. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Lerwill MF, Young RH. Mucinous tumours of the ovary. Diagnostic Histopathology 2008;14:366–87. 10.1016/j.mpdhp.2008.06.010 - DOI
-
- Gore M, Hackshaw A, Brady WE, et al. . An International, phase III randomized trial in patients with Mucinous epithelial ovarian cancer (mEOC/GOG 0241) with long-term follow-up: and experience of conducting a clinical trial in a rare gynecological tumor. Gynecol Oncol 2019;153:541–8. 10.1016/j.ygyno.2019.03.256 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
