

Combined oral low-dose cyclophosphamide endocrine therapy may improve clinical response among patients with metastatic breast cancer via Tregs in TLSs
- PMID: 38862586
- PMCID: PMC11166640
- DOI: 10.1038/s41598-024-64042-3
Combined oral low-dose cyclophosphamide endocrine therapy may improve clinical response among patients with metastatic breast cancer via Tregs in TLSs
Abstract
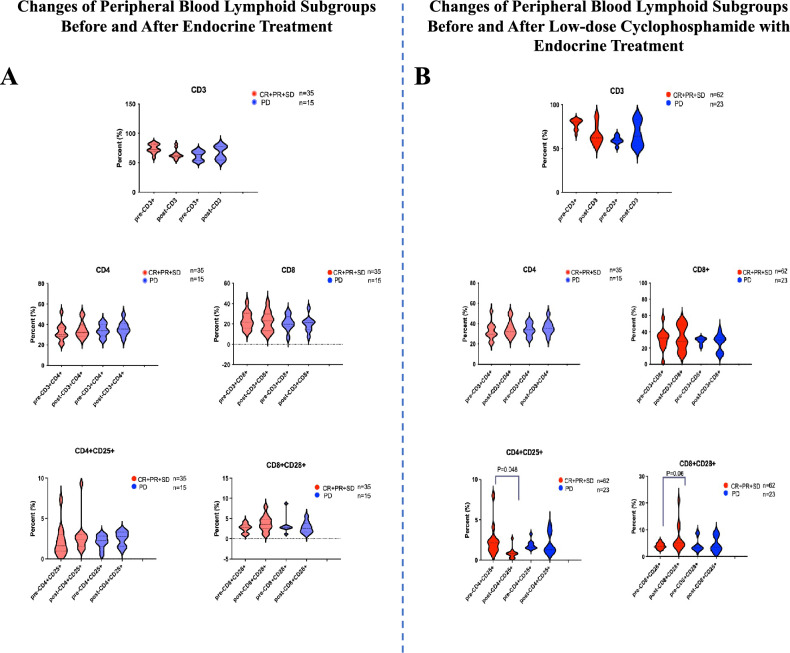
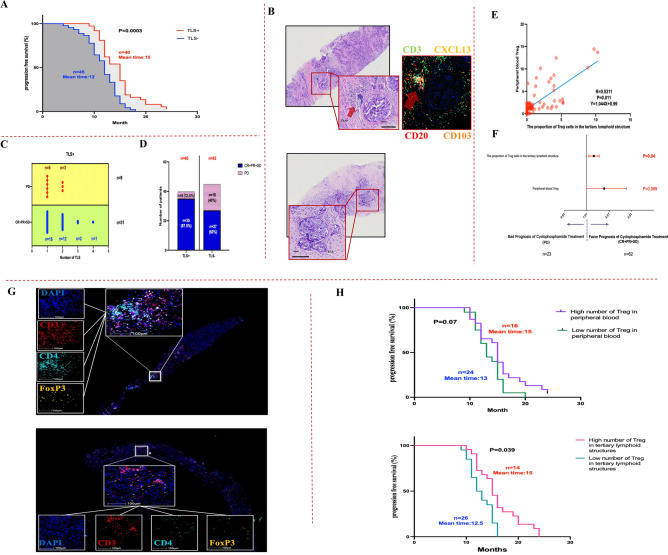
Despite limited research on refractory and/or endocrine therapy failure in elderly metastatic breast cancer (MBC) patients, a prior study showed that low-dose oral cyclophosphamide (CY) can improve the overall survival rate of MBC patients, possibly through the immunoregulation of regulatory T cells (Tregs). We preliminarily investigated the combination of endocrine therapy (ET) with oral low-dose CY as salvage therapy in elderly patients via peripheral blood regulatory T-cell analyses. In addition, we evaluated the associations of tumor tertiary lymphoid structures (TLSs) with therapeutic outcomes. HR+/HER2- advanced breast cancer patients who received low-dose CY combined with ET or ET only from April 2015 to August 2021 were enrolled in this retrospective study. The primary outcome was the clinical control rate (CCR), and the secondary outcome was progression-free survival (PFS). Circulating T lymphocyte subpopulations represented by Tregs were monitored during treatment by flow cytometry methods. TLSs wereconfirmed by hematoxylin-eosin staining of pretreatment specimens, and CD3, CD4, and Foxp3 were detected using Opal multicolor immunofluorescence. A total of 85 patients who received CY + ET and 50 patients who received ET only were enrolled, the percentage of patients who received CCR was 73% (62/85) vs. 70% (45/50), and the objective response rate (ORR) was 28% (24/85) vs. 24% (12/50). No deaths occurred during the study period. The mean PFS time was 13 vs. 11 months (P = 0.03). In the CY + ET group, decreases in CD4+/CD25+/Foxp3+ T cells (P < 0.001) were favorable for both clinical control and prolonged PFS (P < 0.001). Compared with patients without TLSs, those with TLSs were more likely to have better clinical control and PFS (mean time = 6 months), and a greater number of Treg cells during TLS pretreatment correlated with longer PFS (P = 0.043). Oral low-dose CY combined with standard ET exerts immunological effects by decreasing Treg levels to achieve improved clinical responses. Moreover, patients with TLSs might benefit more from such therapy than those without TLSs, and a high Treg cell count in TLSs before treatment predicts better therapeutic efficacy.
Keywords: Cyclophosphamide; Low dose; Metastatic breast cancer; Regulatory T cell; Tertiary lymphoid structures; Tumor microenvironment.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Serial immunological parameters in a phase II trial of exemestane and low-dose oral cyclophosphamide in advanced hormone receptor-positive breast cancer.Breast Cancer Res Treat. 2018 Feb;168(1):57-67. doi: 10.1007/s10549-017-4570-4. Epub 2017 Nov 9. Breast Cancer Res Treat. 2018. PMID: 29124456 Clinical Trial.
-
Metronomic cyclophosphamide treatment in metastasized breast cancer patients: immunological effects and clinical outcome.Cancer Immunol Immunother. 2012 Mar;61(3):353-62. doi: 10.1007/s00262-011-1106-3. Epub 2011 Sep 14. Cancer Immunol Immunother. 2012. PMID: 21915801 Free PMC article. Clinical Trial.
-
Pertuzumab and trastuzumab with or without metronomic chemotherapy for older patients with HER2-positive metastatic breast cancer (EORTC 75111-10114): an open-label, randomised, phase 2 trial from the Elderly Task Force/Breast Cancer Group.Lancet Oncol. 2018 Mar;19(3):323-336. doi: 10.1016/S1470-2045(18)30083-4. Epub 2018 Feb 9. Lancet Oncol. 2018. PMID: 29433963 Clinical Trial.
-
The Presence of Tertiary Lymphoid Structures Provides New Insight Into the Clinicopathological Features and Prognosis of Patients With Breast Cancer.Front Immunol. 2022 May 19;13:868155. doi: 10.3389/fimmu.2022.868155. eCollection 2022. Front Immunol. 2022. PMID: 35664009 Free PMC article.
-
Regulatory T-cell modulation using cyclophosphamide in vaccine approaches: a current perspective.Cancer Res. 2012 Jul 15;72(14):3439-44. doi: 10.1158/0008-5472.CAN-11-3912. Epub 2012 Jul 3. Cancer Res. 2012. PMID: 22761338 Free PMC article. Review.
Cited by
-
[Chinese Expert Consensus on Assessment and Clinical Application of Tertiary Lymphoid Structure for Non-small Cell Lung Cancer (2025 Version)].Zhongguo Fei Ai Za Zhi. 2025 Feb 20;28(2):95-104. doi: 10.3779/j.issn.1009-3419.2025.102.03. Zhongguo Fei Ai Za Zhi. 2025. PMID: 40114486 Free PMC article. Review. Chinese.
-
Prodrugs in Oncology: Bioactivation and Impact on Therapeutic Efficacy and Toxicity.Int J Mol Sci. 2025 Jan 24;26(3):988. doi: 10.3390/ijms26030988. Int J Mol Sci. 2025. PMID: 39940757 Free PMC article. Review.
References
-
- Rose C, Vtoraya O, Pluzanska A, Davidson N, Gershanovich M, Thomas R, et al. An open randomised trial of second-line endocrine therapy in advanced breast cancer comparison of the aromatase inhibitors letrozole and anastrozole. Eur. J. Cancer. 2003;39:2318–2327. doi: 10.1016/S0959-8049(03)00630-0. - DOI - PubMed
-
- Chia S, Gradishar W, Mauriac L, Bines J, Amant F, Federico M, et al. Double-blind, randomized placebo controlled trial of fulvestrant compared with exemestane after prior nonsteroidal aromatase inhibitor therapy in postmenopausal women with hormone receptor-positive, advanced breast cancer: results from EFECT. J. Clin. Oncol. 2008;26:1664–1670. doi: 10.1200/JCO.2007.13.5822. - DOI - PubMed
-
- Di Leo A, Jerusalem G, Petruzelka L, Torres R, Bondarenko IN, Khasanov R, et al. Results of the CONFIRM phase III trial comparing fulvestrant 250 mg with fulvestrant 500 mg in postmenopausal women with estrogen receptor-positive advanced breast cancer. J. Clin. Oncol. 2010;28:4594–4600. doi: 10.1200/JCO.2010.28.8415. - DOI - PubMed
-
- Thurlimann B, Robertson JF, Nabholtz JM, Buzdar A, Bonneterre J, Arimidex Study Group Efficacy of tamoxifen following anastrozole (‘Arimidex’) compared with anastrozole following tamoxifen as first-line treatment for advanced breast cancer in postmenopausal women. Eur. J. Cancer. 2003;39:2310–2317. doi: 10.1016/S0959-8049(03)00602-6. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
