

A systematic review and meta-analysis, investigating dose and time of fluvoxamine treatment efficacy for COVID-19 clinical deterioration, death, and Long-COVID complications
- PMID: 38862591
- PMCID: PMC11166997
- DOI: 10.1038/s41598-024-64260-9
A systematic review and meta-analysis, investigating dose and time of fluvoxamine treatment efficacy for COVID-19 clinical deterioration, death, and Long-COVID complications
Erratum in
-
Author Correction: A systematic review and meta-analysis, investigating dose and time of fluvoxamine treatment efficacy for COVID-19 clinical deterioration, death, and Long-COVID complications.Sci Rep. 2024 Jul 22;14(1):16774. doi: 10.1038/s41598-024-67936-4. Sci Rep. 2024. PMID: 39039269 Free PMC article. No abstract available.
Abstract
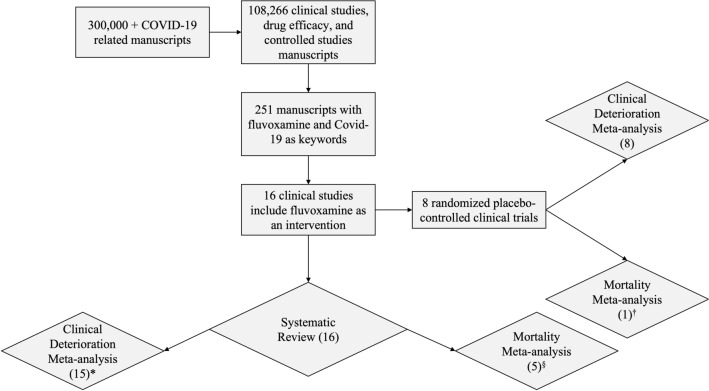
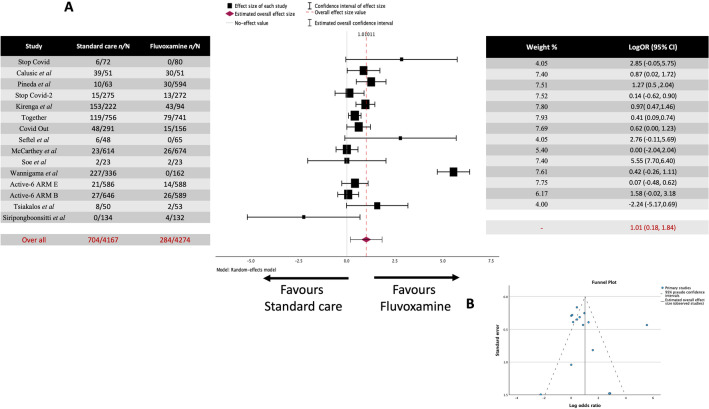
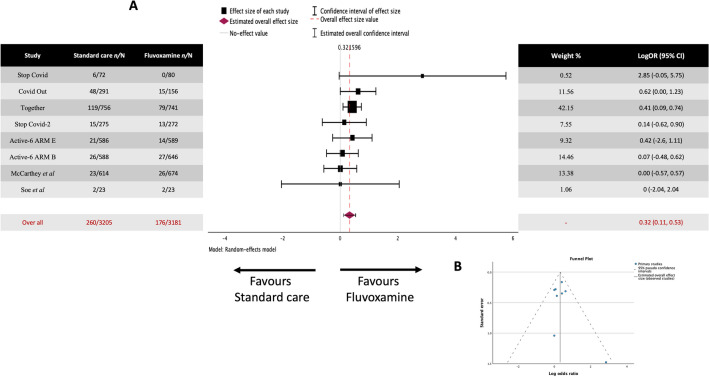
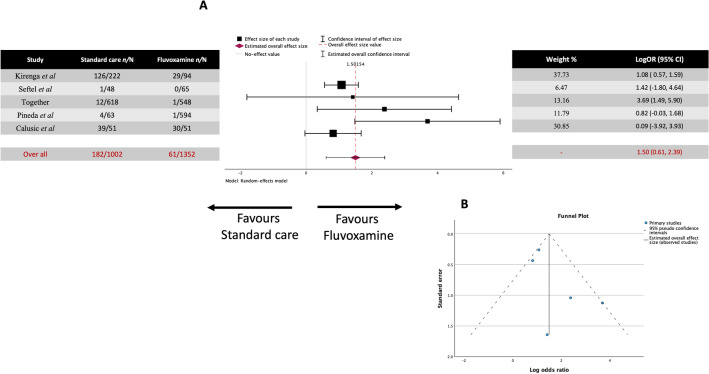
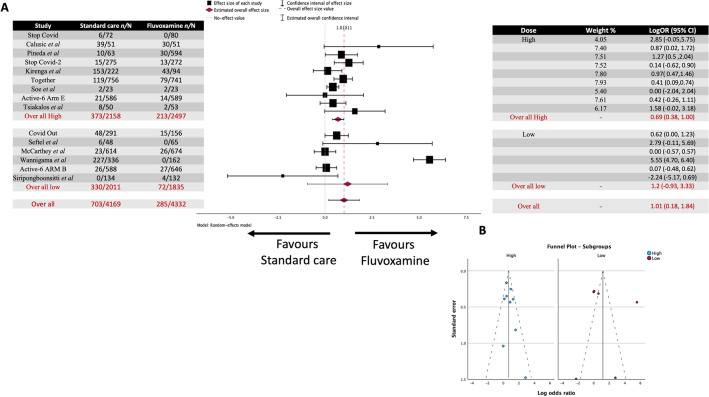
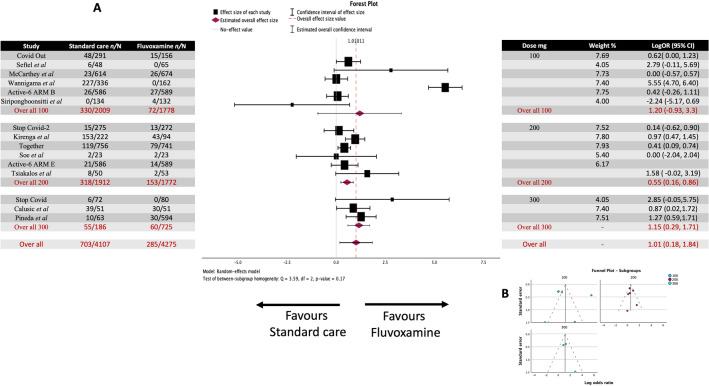
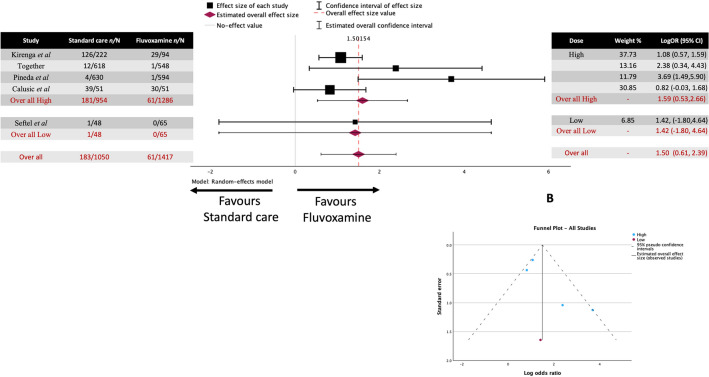
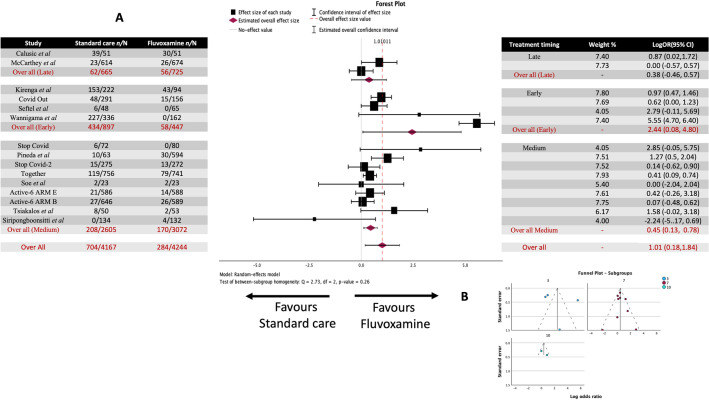
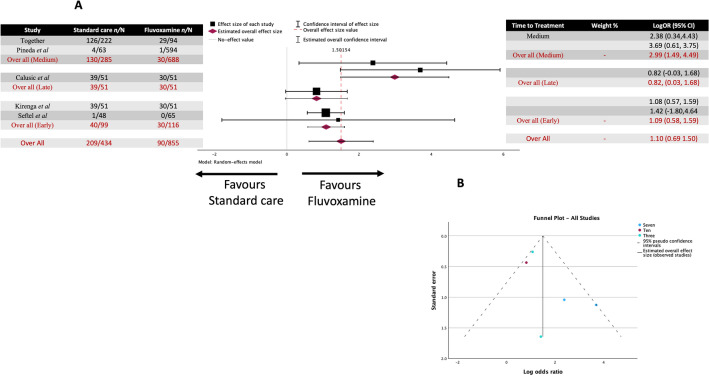
There have been 774,075,242 cases of COVID-19 and 7,012,986 deaths worldwide as of January 2024. In the early stages of the pandemic, there was an urgent need to reduce the severity of the disease and prevent the need for hospitalization to avoid stress on healthcare systems worldwide. The repurposing of drugs to prevent clinical deterioration of COVID-19 patients was trialed in many studies using many different drugs. Fluvoxamine (an SSRI and sigma-1 receptor agonist) was initially identified to potentially provide beneficial effects in COVID-19-infected patients, preventing clinical deterioration and the need for hospitalization. Fourteen clinical studies have been carried out to date, with seven of those being randomized placebo-controlled studies. This systematic review and meta-analysis covers the literature from the outbreak of SARS-CoV-2 in late 2019 until January 2024. Search terms related to fluvoxamine, such as its trade names and chemical names, along with words related to COVID-19, such as SARS-CoV-2 and coronavirus, were used in literature databases including PubMed, Google Scholar, Scopus, and the ClinicalTrials.gov database from NIH, to identify the trials used in the subsequent analysis. Clinical deterioration and death data were extracted from these studies where available and used in the meta-analysis. A total of 7153 patients were studied across 14 studies (both open-label and double-blind placebo-controlled). 681 out of 3553 (19.17%) in the standard care group and 255 out of 3600 (7.08%) in the fluvoxamine-treated group experienced clinical deterioration. The estimated average log odds ratio was 1.087 (95% CI 0.200 to 1.973), which differed significantly from zero (z = 2.402, p = 0.016). The seven placebo-controlled studies resulted in a log odds ratio of 0.359 (95% CI 0.1111 to 0.5294), which differed significantly from zero (z = 3.103, p = 0.002). The results of this study identified fluvoxamine as effective in preventing clinical deterioration, and subgrouping analysis suggests that earlier treatment with a dose of 200 mg or above provides the best outcomes. We hope the outcomes of this study can help design future studies into respiratory viral infections and potentially improve clinical outcomes.
Keywords: (E)‐5‐methoxy‐1‐[4‐(trifluoromethyl)phenyl]pentan‐1‐one O‐2‐aminoethyl oxime); Antidepressant; Coronavirus; Drug repurposing; Pandemic; SARS-CoV-2; Sigma-1 receptor (σ1R).
© 2024. The Author(s).
Conflict of interest statement
AMR is listed as an inventor on a patent application related to methods of treating COVID-19 (including Sigma1 agonists and specifically fluvoxamine), which was filed by Washington University in St. Louis. No other author declares any potential conflict of interest or competing financial or non-financial interest in relation to the manuscript. AMR is listed on a patent application that includes the use of σ1R agonists for the treatment of COVID-19. No other authors have any conflicts to declare.
Figures
References
-
- World-Health-Organization. WHO Coronavirus (COVID-19) Dashboard. WHO Coronavirus (COVID-19), https://data.who.int/dashboards/covid19/deaths (2023).
-
- Suryasa, I. W., Rodríguez-Gámez, M. & Koldoris, T. The COVID-19 pandemic. Int. J. Health Sci.5 (2021).
-
- Wannigama, D. L. et al. Tracing the new SARS-CoV-2 variant BA. 2.86 in the community through wastewater surveillance in Bangkok, Thailand. Lancet Infect. Dis.23, e464–e466 (2023). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
