

Development and validation of a machine learning-based readmission risk prediction model for non-ST elevation myocardial infarction patients after percutaneous coronary intervention
- PMID: 38862634
- PMCID: PMC11166920
- DOI: 10.1038/s41598-024-64048-x
Development and validation of a machine learning-based readmission risk prediction model for non-ST elevation myocardial infarction patients after percutaneous coronary intervention
Abstract
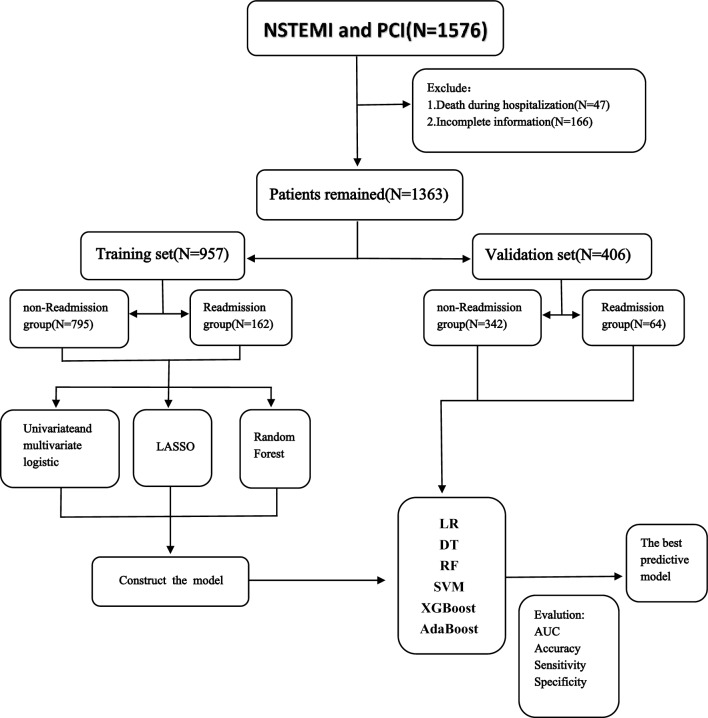
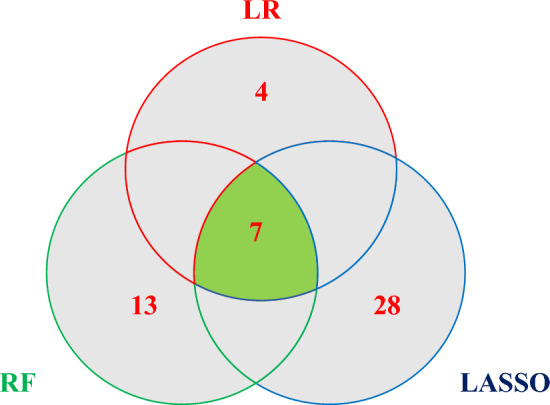
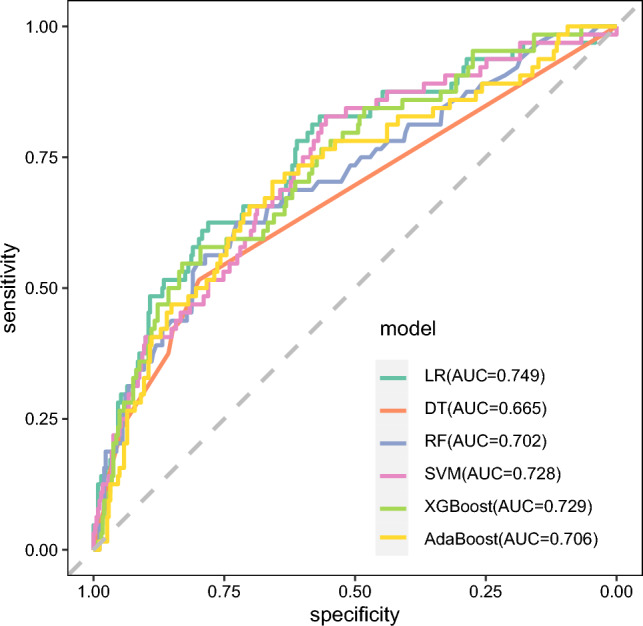
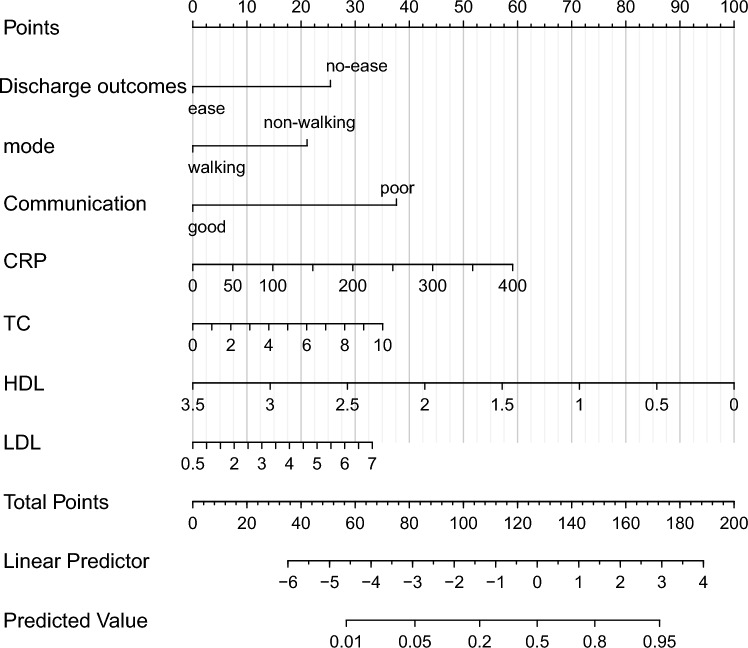
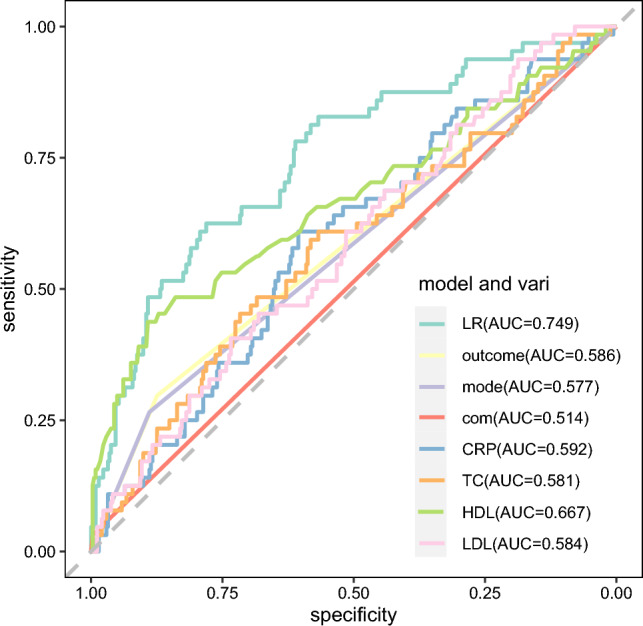
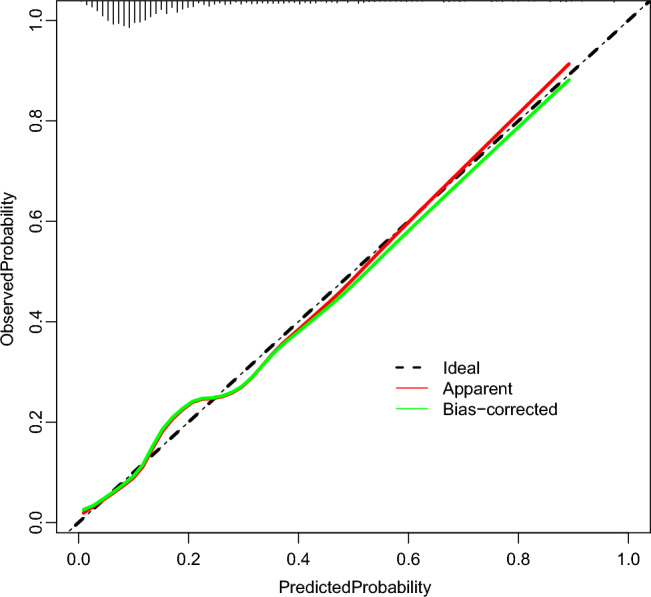
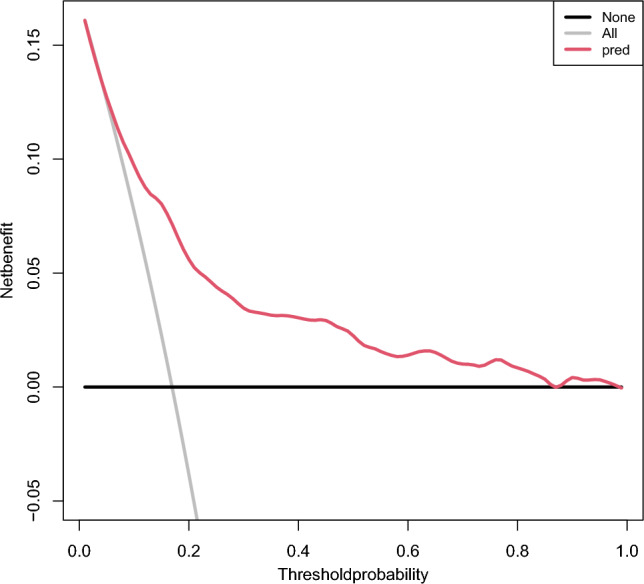
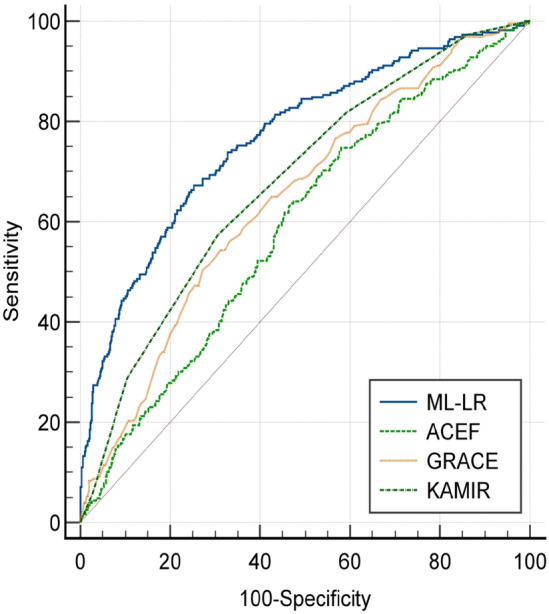
To investigate the factors that influence readmissions in patients with acute non-ST elevation myocardial infarction (NSTEMI) after percutaneous coronary intervention (PCI) by using multiple machine learning (ML) methods to establish a predictive model. In this study, 1576 NSTEMI patients who were hospitalized at the Affiliated Hospital of North Sichuan Medical College were selected as the research subjects. They were divided into two groups: the readmitted group and the non-readmitted group. The division was based on whether the patients experienced complications or another incident of myocardial infarction within one year after undergoing PCI. Common variables selected by univariate and multivariate logistic regression, LASSO regression, and random forest were used as independent influencing factors for NSTEMI patients' readmissions after PCI. Six different ML models were constructed using these common variables. The area under the ROC curve, accuracy, sensitivity, and specificity were used to evaluate the performance of the six ML models. Finally, the optimal model was selected, and a nomogram was created to visually represent its clinical effectiveness. Three different methods were used to select seven representative common variables. These variables were then utilized to construct six different ML models, which were subsequently compared. The findings indicated that the LR model exhibited the most optimal performance in terms of AUC, accuracy, sensitivity, and specificity. The outcome, admission mode (walking and non-walking), communication ability, CRP, TC, HDL, and LDL were identified as independent predicators of readmissions in NSTEMI patients after PCI. The prediction model constructed by the LR algorithm was the best. The established column graph model established proved to be effective in identifying high-risk groups with high accuracy and differentiation. It holds a specific predictive value for the occurrence of readmissions after direct PCI in NSTEMI patients.
Keywords: Machine learning; Non-ST elevation myocardial infarction; PCI; Prediction model; Readmissions.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Development and validation of an AMR-based predictive model for post-PCI upper gastrointestinal bleeding in NSTEMI patients.Front Endocrinol (Lausanne). 2025 Apr 16;16:1545462. doi: 10.3389/fendo.2025.1545462. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40309439 Free PMC article.
-
Association between anaemia and long-term prognosis in patients with non-ST segment elevation myocardial infarction.Acta Cardiol. 2024 Apr;79(2):179-186. doi: 10.1080/00015385.2023.2289718. Epub 2023 Dec 12. Acta Cardiol. 2024. PMID: 38085221
-
Machine learning for predicting intrahospital mortality in ST-elevation myocardial infarction patients with type 2 diabetes mellitus.BMC Cardiovasc Disord. 2023 Nov 27;23(1):585. doi: 10.1186/s12872-023-03626-9. BMC Cardiovasc Disord. 2023. PMID: 38012550 Free PMC article.
-
Twelve-month clinical outcomes of acute non-ST versus ST-segment elevation myocardial infarction patients with reduced preprocedural thrombolysis in myocardial infarction flow undergoing percutaneous coronary intervention.Coron Artery Dis. 2018 Aug;29(5):416-422. doi: 10.1097/MCA.0000000000000632. Coron Artery Dis. 2018. PMID: 29708887
-
A Predictive Model for Contrast-Induced Acute Kidney Injury After Percutaneous Coronary Intervention in Elderly Patients with ST-Segment Elevation Myocardial Infarction.Clin Interv Aging. 2023 Mar 22;18:453-465. doi: 10.2147/CIA.S402408. eCollection 2023. Clin Interv Aging. 2023. PMID: 36987461 Free PMC article. Clinical Trial.
Cited by
-
Predictive and prognostic nomogram models for liver metastasis in colorectal neuroendocrine neoplasms: a large population study.Front Endocrinol (Lausanne). 2025 Jan 7;15:1488733. doi: 10.3389/fendo.2024.1488733. eCollection 2024. Front Endocrinol (Lausanne). 2025. PMID: 39839478 Free PMC article.
-
Risk factors and prediction model for carbapenem-resistant organism infection in sepsis patients.Eur J Med Res. 2025 Mar 25;30(1):201. doi: 10.1186/s40001-025-02448-z. Eur J Med Res. 2025. PMID: 40128899 Free PMC article.
-
Comparing the Performance of Machine Learning Models and Conventional Risk Scores for Predicting Major Adverse Cardiovascular Cerebrovascular Events After Percutaneous Coronary Intervention in Patients With Acute Myocardial Infarction: Systematic Review and Meta-Analysis.J Med Internet Res. 2025 Jul 18;27:e76215. doi: 10.2196/76215. J Med Internet Res. 2025. PMID: 40680235 Free PMC article.
References
-
- Writing committee of the report on cardiovascular health and diseases in China. Interpretation of report on cardiovascular health and diseases in China 2021. Chin. J. Cardiovasc. Med. 27(04): 305–318 (2022).
-
- Desai NR, Ross JS, Kwon JY, Herrin J, Dharmarajan K, Bernheim SM, Krumholz HM, Horwitz LI. Association between hospital penalty status under the hospital readmission reduction program and readmission rates for target and nontarget conditions. JAMA. 2016;316(24):2647–2656. doi: 10.1001/jama.2016.18533. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- 2022ZYD0056/the Central Government Guides Local Scientific and Technological Development Projects
- 23JCYJPT0059/the Nanchong science and technology plan project
- CBY23-TD01/Research and development program of North Sichuan Medical College
- YCH-KY-YCZD2024-015/Sichuan Medical Science and Technology Innovation Research Society Program
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
