

Navigated intraoperative ultrasound in pediatric brain tumors
- PMID: 38862795
- PMCID: PMC11322494
- DOI: 10.1007/s00381-024-06492-8
Navigated intraoperative ultrasound in pediatric brain tumors
Erratum in
-
Correction: Navigated intraoperative ultrasound in pediatric brain tumors.Childs Nerv Syst. 2025 Apr 14;41(1):156. doi: 10.1007/s00381-025-06824-2. Childs Nerv Syst. 2025. PMID: 40227464 Free PMC article. No abstract available.
Abstract
Purpose: The aim of this study was to evaluate the diagnostic value and accuracy of navigated intraoperative ultrasound (iUS) in pediatric oncological neurosurgery as compared to intraoperative magnetic resonance imaging (iMRI).
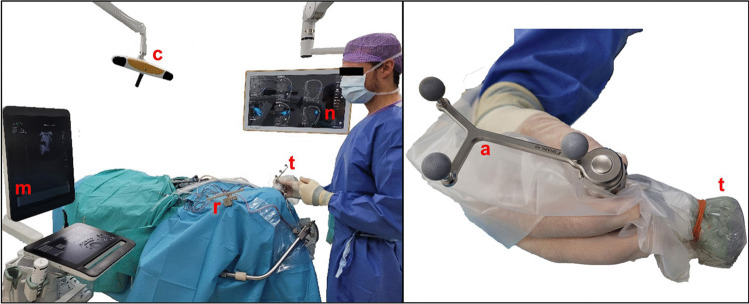
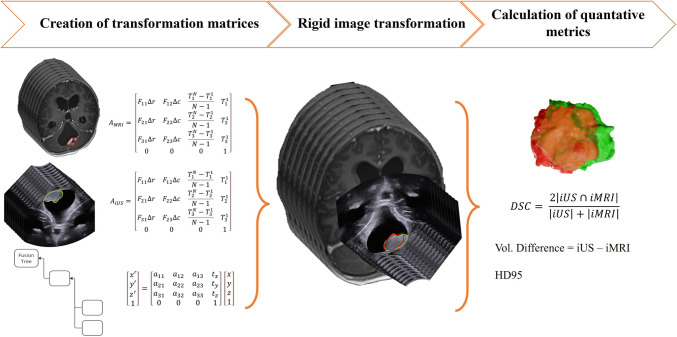
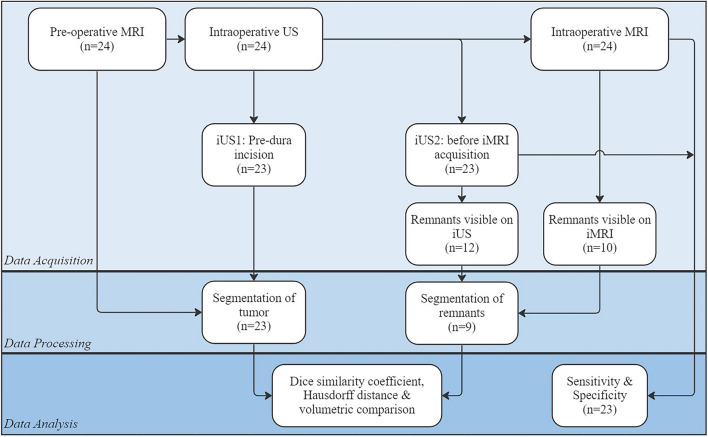
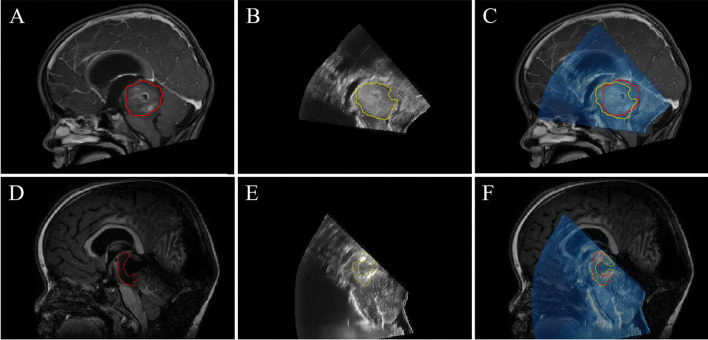
Methods: A total of 24 pediatric patients undergoing tumor debulking surgery with iUS, iMRI, and neuronavigation were included in this study. Prospective acquisition of iUS images was done at two time points during the surgical procedure: (1) before resection for tumor visualization and (2) after resection for residual tumor assessment. Dice similarity coefficients (DSC), Hausdorff distances 95th percentiles (HD95) and volume differences, sensitivity, and specificity were calculated for iUS segmentations as compared to iMRI.
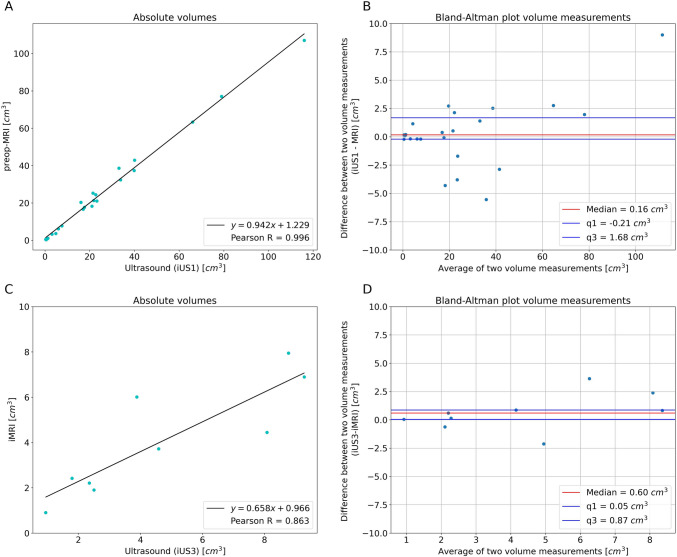
Results: A high correlation (R = 0.99) was found for volume estimation as measured on iUS and iMRI before resection. A good spatial accuracy was demonstrated with a median DSC of 0.72 (IQR 0.14) and a median HD95 percentile of 4.98 mm (IQR 2.22 mm). The assessment after resection demonstrated a sensitivity of 100% and a specificity of 84.6% for residual tumor detection with navigated iUS. A moderate accuracy was observed with a median DSC of 0.58 (IQR 0.27) and a median HD95 of 5.84 mm (IQR 4.04 mm) for residual tumor volumes.
Conclusion: We found that iUS measurements of tumor volume before resection correlate well with those obtained from preoperative MRI. The accuracy of residual tumor detection was reliable as compared to iMRI, indicating the suitability of iUS for directing the surgeon's attention to areas suspect for residual tumor. Therefore, iUS is considered as a valuable addition to the neurosurgical armamentarium.
Trial registration number and date: PMCLAB2023.476, February 12th 2024.
Keywords: Brain tumor; Intraoperative MRI; Intraoperative ultrasound; Navigation; Pediatrics.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Navigated Intraoperative Ultrasound Offers Effective and Efficient Real-Time Analysis of Intracranial Tumor Resection and Brain Shift.Oper Neurosurg. 2025 Feb 1;28(2):148-158. doi: 10.1227/ons.0000000000001250. Epub 2024 Jul 12. Oper Neurosurg. 2025. PMID: 38995025
-
Role of intraoperative ultrasound and MRI to aid grade of resection of pediatric low-grade gliomas: accumulated experience from 4 centers.Childs Nerv Syst. 2024 Oct;40(10):3165-3172. doi: 10.1007/s00381-024-06532-3. Epub 2024 Jul 16. Childs Nerv Syst. 2024. PMID: 39012356
-
Intraoperative ultrasound in pediatric brain tumors: does the surgeon get it right?Childs Nerv Syst. 2015 Dec;31(12):2353-7. doi: 10.1007/s00381-015-2805-4. Epub 2015 Aug 5. Childs Nerv Syst. 2015. PMID: 26243159
-
Reliability of intraoperative ultrasound in detecting tumor residual after brain diffuse glioma surgery: a systematic review and meta-analysis.Neurosurg Rev. 2020 Oct;43(5):1221-1233. doi: 10.1007/s10143-019-01160-x. Epub 2019 Aug 14. Neurosurg Rev. 2020. PMID: 31410683
-
Neurosurgical tools to extend tumor resection in pediatric hemispheric low-grade gliomas: iMRI.Childs Nerv Syst. 2016 Oct;32(10):1915-22. doi: 10.1007/s00381-016-3177-0. Epub 2016 Sep 20. Childs Nerv Syst. 2016. PMID: 27659833 Review.
Cited by
-
Advancements in Imaging and Neurosurgical Techniques for Brain Tumor Resection: A Comprehensive Review.Cureus. 2024 Oct 31;16(10):e72745. doi: 10.7759/cureus.72745. eCollection 2024 Oct. Cureus. 2024. PMID: 39618625 Free PMC article. Review.
References
-
- Udaka YT, Packer RJ (2018) Pediatric brain tumors. Neurol Clin 36(3):533–556. 10.1016/J.NCL.2018.04.009 - PubMed
-
- Gnekow AK, Kandels D, Van TC et al (2019) SIOP-E-BTG and GPOH guidelines for diagnosis and treatment of children and adolescents with low grade glioma. Klin Padiatr 231(3):107–135. 10.1055/A-0889-8256 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
