

Whole-tumoral metabolic heterogeneity in 18F-FDG PET/CT is a novel prognostic marker for neuroblastoma
- PMID: 38863073
- PMCID: PMC11167917
- DOI: 10.1186/s40644-024-00718-3
Whole-tumoral metabolic heterogeneity in 18F-FDG PET/CT is a novel prognostic marker for neuroblastoma
Abstract
Background: Neuroblastoma (NB) is a highly heterogeneous tumor, and more than half of newly diagnosed NB are associated with extensive metastases. Accurately characterizing the heterogeneity of whole-body tumor lesions remains clinical challenge. This study aims to quantify whole-tumoral metabolic heterogeneity (WMH) derived from whole-body tumor lesions, and investigate the prognostic value of WMH in NB.
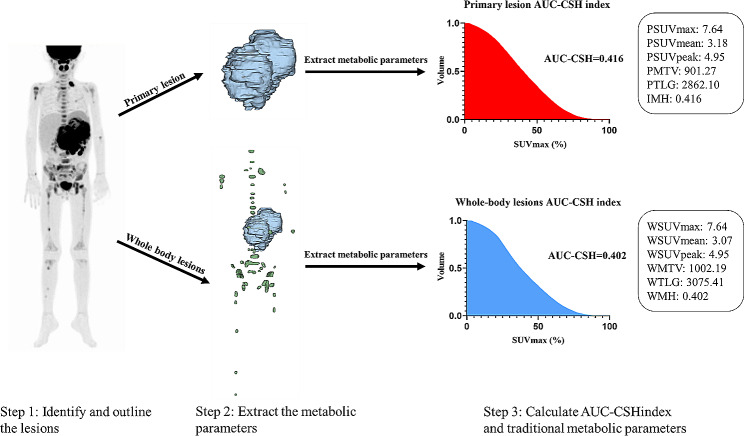
Methods: We retrospectively enrolled 95 newly diagnosed pediatric NB patients in our department. Traditional semi-quantitative PET/CT parameters including the maximum standardized uptake value (SUVmax), the mean standardized uptake value (SUVmean), the peak standardized uptake value (SUVpeak), metabolic tumor volume (MTV) and total lesion glycolysis (TLG) were measured. These PET/CT parameters were expressed as PSUVmax, PSUVmean, PSUVpeak, PMTV, PTLG for primary tumor, WSUVmax, WSUVmean, WSUVpeak, WMTV, WTLG for whole-body tumor lesions. The metabolic heterogeneity was quantified using the areas under the curve of the cumulative SUV-volume histogram index (AUC-CSH index). Intra-tumoral metabolic heterogeneity (IMH) and WMH were extracted from primary tumor and whole-body tumor lesions, respectively. The outcome endpoints were overall survival (OS) and progression-free survival (PFS). Survival analysis was performed utilizing the univariate and multivariate Cox proportional hazards regression. The optimal cut-off values for metabolic parameters were obtained by receiver operating characteristic curve (ROC).
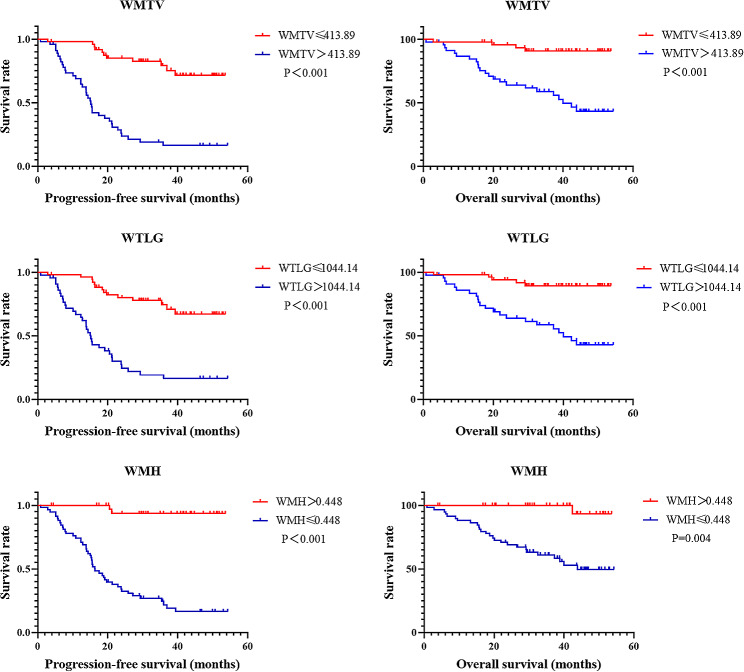
Results: During follow up, 27 (28.4%) patients died, 21 (22.1%) patients relapsed and 47 (49.5%) patients remained progression-free survival, with a median follow-up of 35.0 months. In survival analysis, WMTV and WTLG were independent indicators of PFS, and WMH was an independent risk factor of PFS and OS. However, IMH only showed association with PFS and OS. In addition to metabolic parameters, the International Neuroblastoma Staging System (INSS) was identified as an independent risk factor for PFS, and neuron-specific enolase (NSE) served as an independent predictor of OS.
Conclusion: WMH was an independent risk factor for PFS and OS, suggesting its potential as a novel prognostic marker for newly diagnosed NB patients.
Keywords: 18F-FDG PET/CT; Intra-tumoral metabolic heterogeneity; Neuroblastoma; Prognosis; Whole-tumoral metabolic heterogeneity.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Value of pretreatment 18F-FDG PET/CT in prognosis and the reflection of tumor burden: a study in pediatric patients with newly diagnosed neuroblastoma.Int J Med Sci. 2021 Feb 24;18(8):1857-1865. doi: 10.7150/ijms.58263. eCollection 2021. Int J Med Sci. 2021. PMID: 33746603 Free PMC article.
-
The prognostic value of 18F-FDG PET/CT intra-tumoural metabolic heterogeneity in pretreatment neuroblastoma patients.Cancer Imaging. 2022 Jul 5;22(1):32. doi: 10.1186/s40644-022-00472-4. Cancer Imaging. 2022. PMID: 35791003 Free PMC article.
-
Prognostic Value of Volume-Based Metabolic Parameters Obtained by 18F-FDG-PET/CT in Patients With Locally Advanced Squamous Cell Cervical Carcinoma.J Comput Assist Tomogr. 2018 May/Jun;42(3):429-434. doi: 10.1097/RCT.0000000000000708. J Comput Assist Tomogr. 2018. PMID: 29369948
-
Prognostic prediction by 18F-FDG-PET/CT parameters in patients with neuroblastoma: a systematic review and meta-analysis.Front Oncol. 2023 Jul 14;13:1208531. doi: 10.3389/fonc.2023.1208531. eCollection 2023. Front Oncol. 2023. PMID: 37519817 Free PMC article.
-
Recommendations for the use of nuclear medicine imaging in patients with neuroblastoma.Clin Transl Oncol. 2025 Jun;27(6):2401-2415. doi: 10.1007/s12094-024-03755-3. Epub 2024 Nov 7. Clin Transl Oncol. 2025. PMID: 39508974 Review.
Cited by
-
The baseline 18F-FDG PET/CT imaging features in pediatric patients with congenital neuroblastoma.BMC Med Imaging. 2025 Aug 14;25(1):330. doi: 10.1186/s12880-025-01863-2. BMC Med Imaging. 2025. PMID: 40813959 Free PMC article.
-
18F-FDG PET/CT Radiomics for Predicting Therapy Response in Primary Mediastinal B-Cell Lymphoma: A Bi-Centric Pilot Study.Cancers (Basel). 2025 May 30;17(11):1827. doi: 10.3390/cancers17111827. Cancers (Basel). 2025. PMID: 40507310 Free PMC article.
References
-
- Ward E, DeSantis C, Robbins A et al. Childhood and adolescent cancer statistics, 2014. CA: a cancer journal for clinicians. 2014 Mar-Apr;64(2):83–103. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
