

FAS(APO), DAMP, and AKT Phosphoproteins Expression Predict the Development of Nosocomial Infection After Pediatric Burn Injury
- PMID: 38863248
- PMCID: PMC11565198
- DOI: 10.1093/jbcr/irae111
FAS(APO), DAMP, and AKT Phosphoproteins Expression Predict the Development of Nosocomial Infection After Pediatric Burn Injury
Abstract
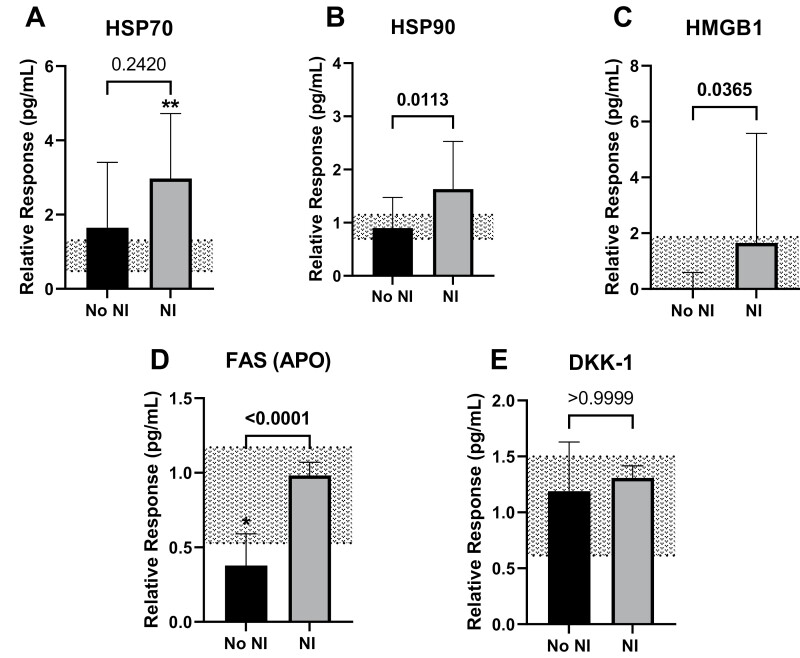
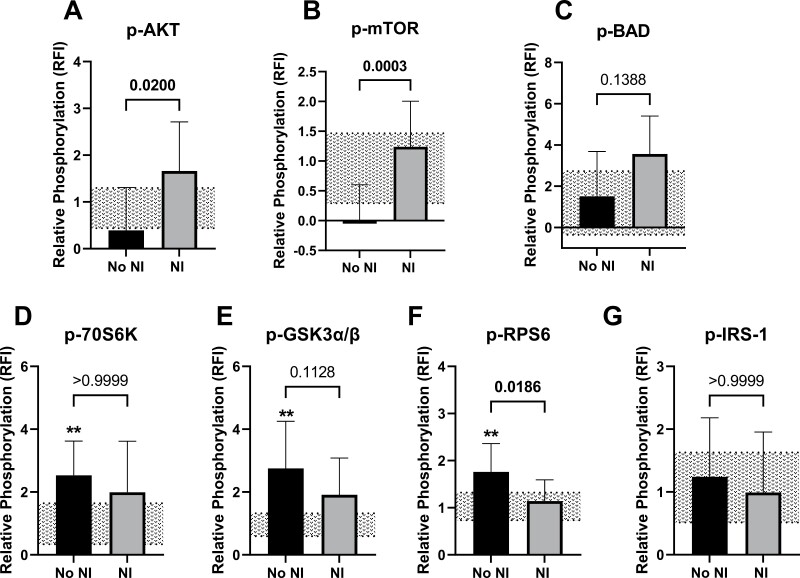
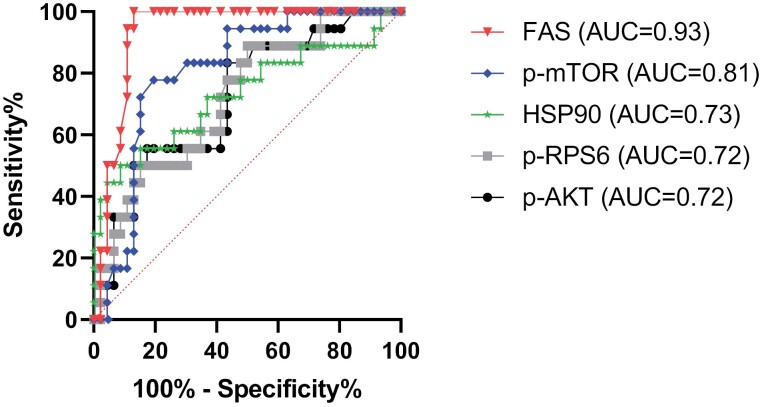
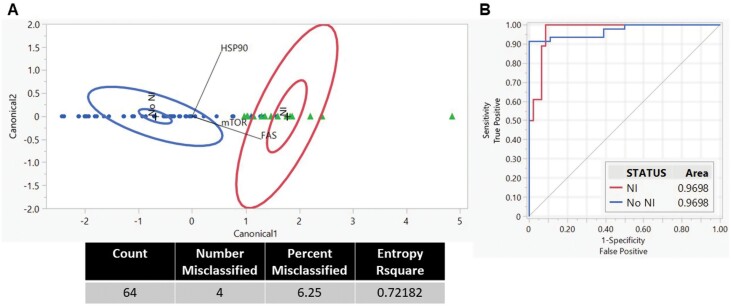
Pediatric burn injuries are a leading cause of morbidity with infections being the most common acute complication. Thermal injuries elicit a heightened cytokine response while suppressing immune function; however, the mechanisms leading to this dysfunction are still unknown. Our aim was to identify extracellular proteins and circulating phosphoprotein expression in the plasma after burn injury to predict the development of nosocomial infection (NI). Plasma was collected within 72 hours after injury from 64 pediatric burn subjects; of these, 18 went on to develop an NI. Extracellular damage-associated molecular proteins, FAS(APO), and protein kinase b (AKT) signaling phosphoproteins were analyzed. Subjects who went on to develop an NI had elevated high-mobility group box 1, heat shock protein 90 (HSP90), and FAS expression than those who did not develop an NI after injury (NoNI). Concurrently, phosphorylated (p-)AKT and mammalian target of rapamycin (p-mTOR) were elevated in those subjects who went on to develop an NI. Quadratic discriminant analysis revealed distinct differential profiles between NI and NoNI burn subjects using HSP90, FAS, and p-mTOR. The area under the receiver-operator characteristic curves displayed significant ability to distinguish between these 2 burn subject cohorts. These findings provide insight into predicting the signaling proteins involved in the development of NI in pediatric burn patients. Further, these proteins show promise as a diagnostic tool for pediatric burn patients at risk of developing infection while additional investigation may lead to potential therapeutics to prevent NI.
Keywords: FAS; danger-associated molecular protein; nosocomial infection; pediatric thermal injury; phosphoprotein.
© The Author(s) 2024. Published by Oxford University Press on behalf of the American Burn Association. All rights reserved. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through our RightsLink service via the Permissions link on the article page on our site—for further information please contact journals.permissions@oup.com.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- American Burn Association. National Burn Repository 2016: Report of Data From 2006-2015. 2017. Accessed 2021. https://ameriburn.org/wp-content/uploads/2017/05/2016abanbr_final_42816.pdf
-
- Gonzalez R, Shanti CM.. Overview of current pediatric burn care. Semin Pediatr Surg. 2015;24(1):47–49. https://doi.org/ 10.1053/j.sempedsurg.2014.11.008 - DOI - PubMed
-
- World Health Organization. Burns. World Health Organization; 2018. Accessed August 5, 2021. https://www.who.int/news-room/fact-sheets/detail/burns
-
- Thakkar RK, Devine R, Popelka J, et al. Measures of systemic innate immune function predict the risk of nosocomial infection in pediatric burn patients. J Burn Care Res. 2020;42(3):488–494. https://doi.org/ 10.1093/jbcr/iraa193 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
