Evaluation of the effects of ectopic replantation on amputate survival in the management of crush traumatic amputations in rats: An experimental study
- PMID: 38863288
- PMCID: PMC11230047
- DOI: 10.14744/tjtes.2024.39470
Evaluation of the effects of ectopic replantation on amputate survival in the management of crush traumatic amputations in rats: An experimental study
Abstract
Background: This controlled experimental study aimed to compare ectopic replantation with other replantation techniques in a rat model of crush amputations. It also assessed the impact of different replantation methods on the viability of amputates.
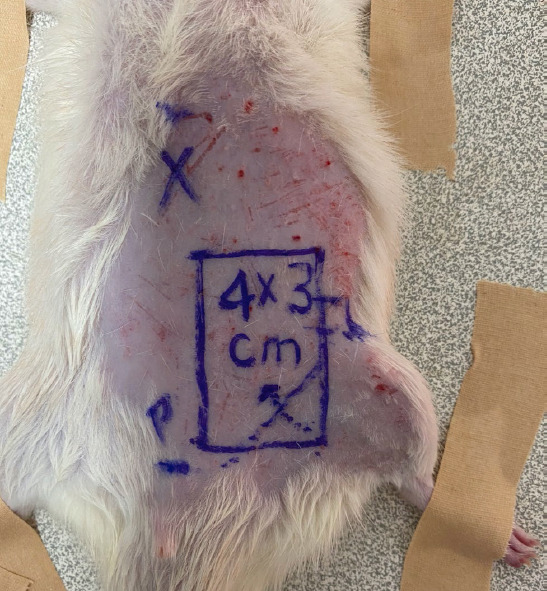
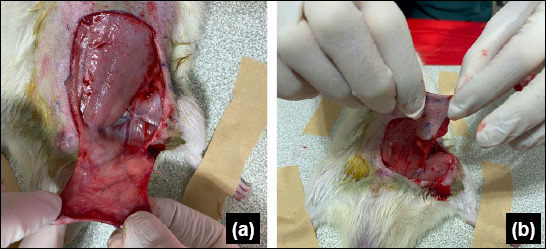
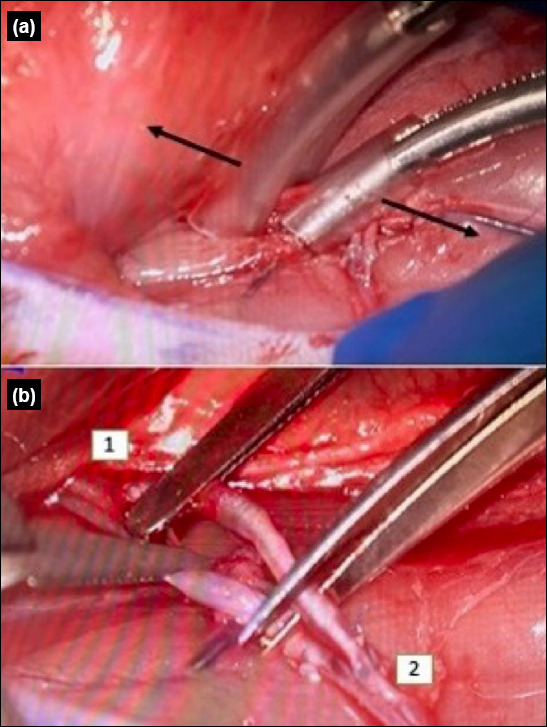
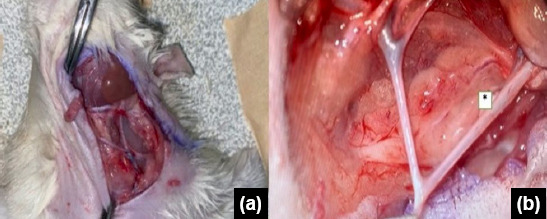
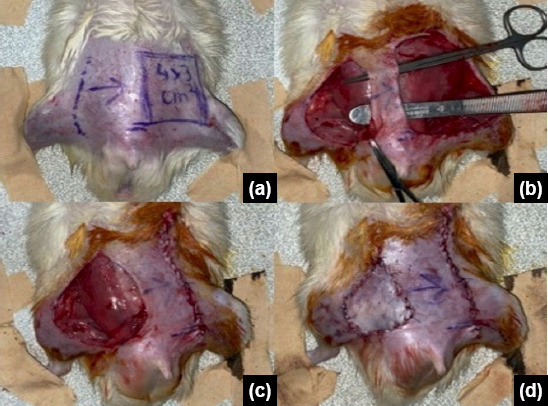
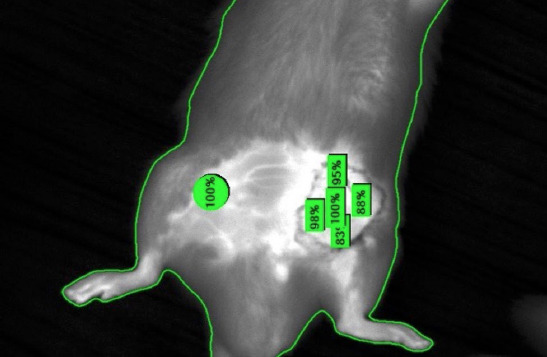
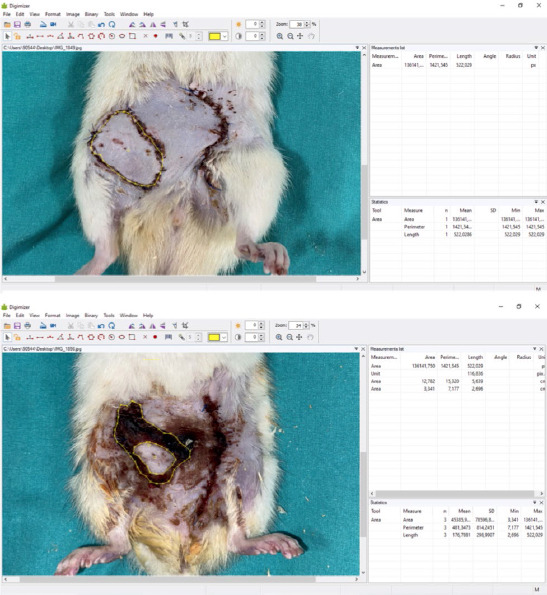
Methods: Forty male Wistar albino rats were divided into four groups. Groin flaps served as the amputation model. Group 1 un-derwent guillotine-style amputation followed by orthotopic replantation, Group 2 experienced crush-type amputation and orthotopic replantation, Group 3 had crush-type amputation and orthotopic replantation with a vein graft, and Group 4 underwent crush-type amputation followed by ectopic replantation. Flap viability and perfusion rates were assessed on day 3 using an infrared perfusion as-sessment system. The ratio of viable area to total flap area and thrombus formation in the pedicle vessels were evaluated on day 7.
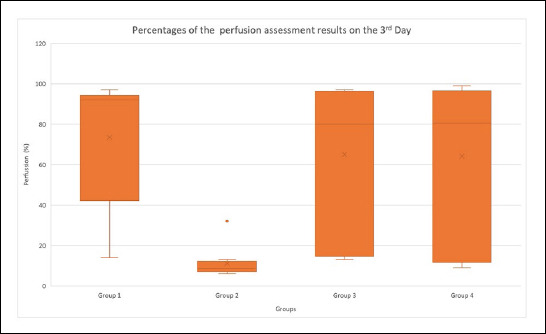
Results: Infrared evaluations on day 3 post-replantation revealed flap perfusion percentages of 73.5% in Group 1, 11.1% in Group 2, 65% in Group 3, and 64.1% in Group 4. Statistical analysis indicated that Group 1 exhibited the highest perfusion rates, while Group 2 showed the lowest. No differences were observed between Groups 3 and 4. On the seventh day, the average surviving flap areas were found to be 74.6% in Group 1, 2.5% in Group 2, 64.5% in Group 3, and 64% in Group 4. Statistically, Group 1 exhibited the best outcomes, while Group 2 had the poorest, with no differences between Groups 3 and 4. Additionally, thrombus formation was observed in the vessels of two animals in Group 1, nine in Group 2, and three each in Groups 3 and 4. Significant statistical differences were noted among the groups.
Conclusion: The results indicate that ectopic replantation and replantation with a vein graft are equally effective. The preferred method for crush-type replantations may depend on the patient's and the amputated limb's conditions. In crush-type amputations, we recommend vein graft repair if the patient's overall condition supports replantation and if crushed segments can be debrided without excessive shortening of the amputated part. If these conditions are not met, temporary ectopic replantation is advised to preserve the amputated limb.
Conflict of interest statement
Figures

References
-
- Pederson WC. Replantation. Plast Reconstr Surg. 2001;107:823–41. - PubMed
-
- An PC, Kuo YR, Lin TS, Yeh MC, Jeng SF. Heterotopic replantation in mutilating hand injury. Ann Plast Surg. 2003;50:113–9. - PubMed
-
- Del Pinal F, Urrutia E, Klich M. Severe crush injury to the forearm and hand:the role of microsurgery. Clin Plast Surg. 2017;44:233–5. - PubMed
-
- Cavadas PC, Landin L, Thione A. Secondary ectopic transfer for replantation salvage after severe wound infection. Microsurg. 2011;31:288–92. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous