

Associations of mid-to-late-life inflammation with late-life mobility and the influences of chronic comorbidities, race, and social determinants of health: The Atherosclerosis Risk in Communities Study
- PMID: 38863338
- PMCID: PMC11323257
- DOI: 10.1111/jgs.18978
Associations of mid-to-late-life inflammation with late-life mobility and the influences of chronic comorbidities, race, and social determinants of health: The Atherosclerosis Risk in Communities Study
Abstract
Background: Relationships of midlife inflammation with late-life mobility and influences of chronic health conditions, race, and social determinants of health (SDoH) on these relationships are poorly understood.
Methods: Among 4758 community-dwelling participants (41% men, 20% Black), high-sensitivity C-reactive protein (hsCRP) was measured over 20+ years: in midlife at study visit 2 (V2: 1990-1992, 47-68 years); at V4 (1996-1998, 53-74 years); and with concurrent late-life 4-m gait speed at V5 (2011-2013, 67-88 years, mean 75 years). SDoH measures included race, the national-rank area deprivation index, education, and income. We examined associations of late-life gait speed with midlife hsCRP (V2 continuous and clinically high ≥3 mg/L), with 20-year hsCRP history from midlife (V2-V5 average continuous hsCRP and clinically high ≥3 mg/L) and with inflammation accumulation (visits and years with high hsCRP). Regression models adjusted for demographic, cardiovascular, and SDoH measures; effect modification by the presence of other common chronic conditions (obesity, diabetes, hypertension) and race were examined, with and without accounting for SDoH.
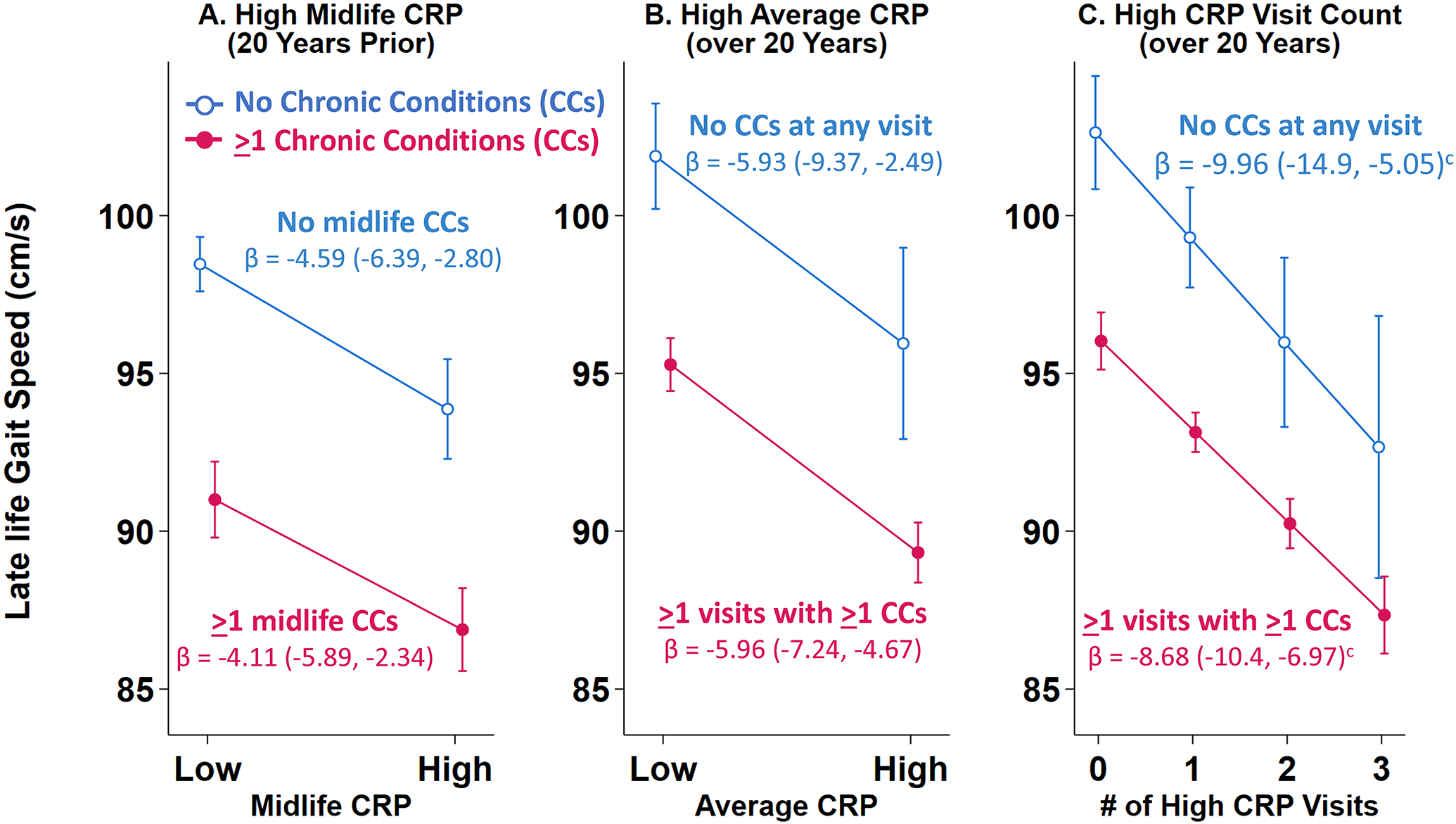
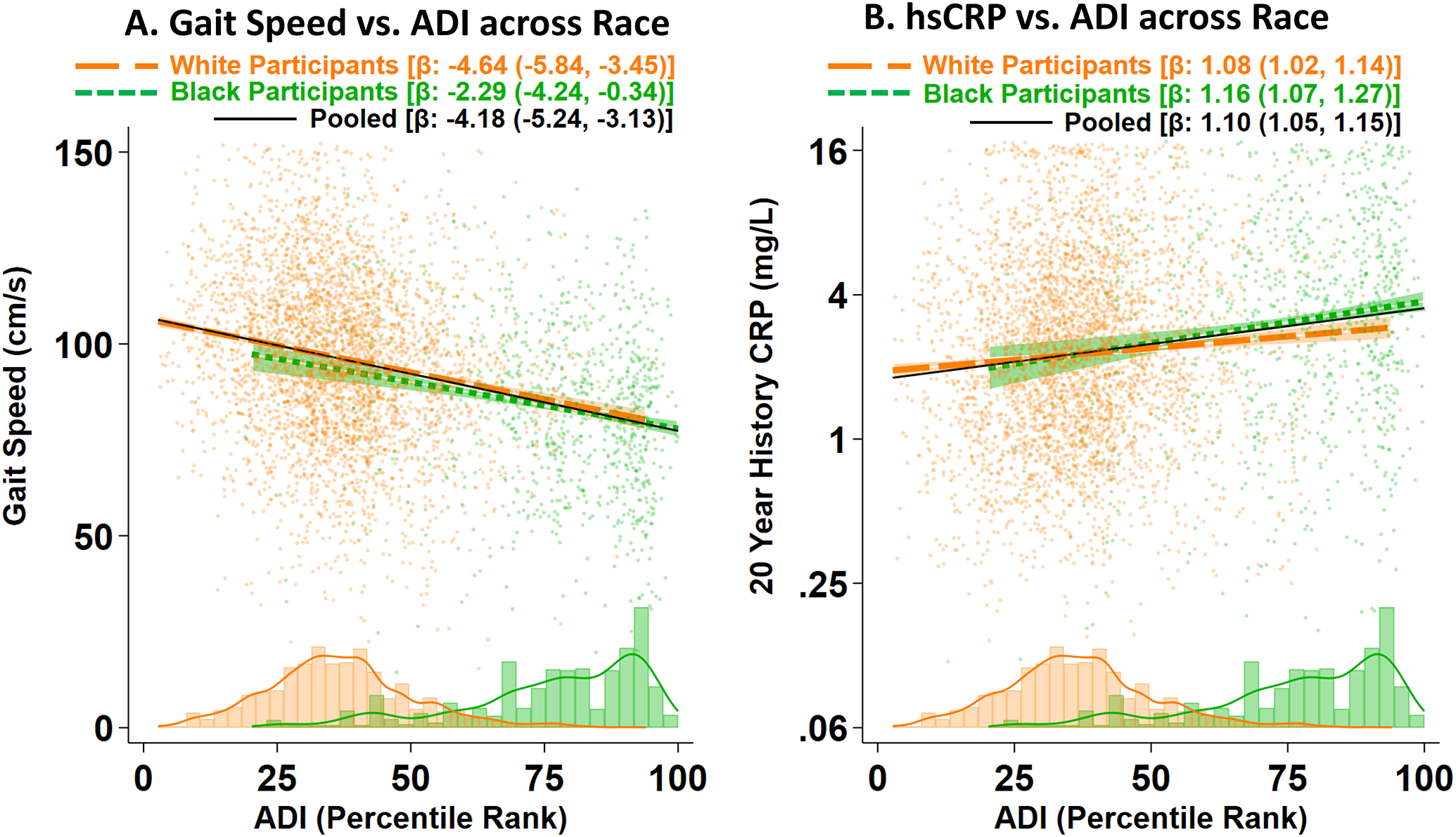
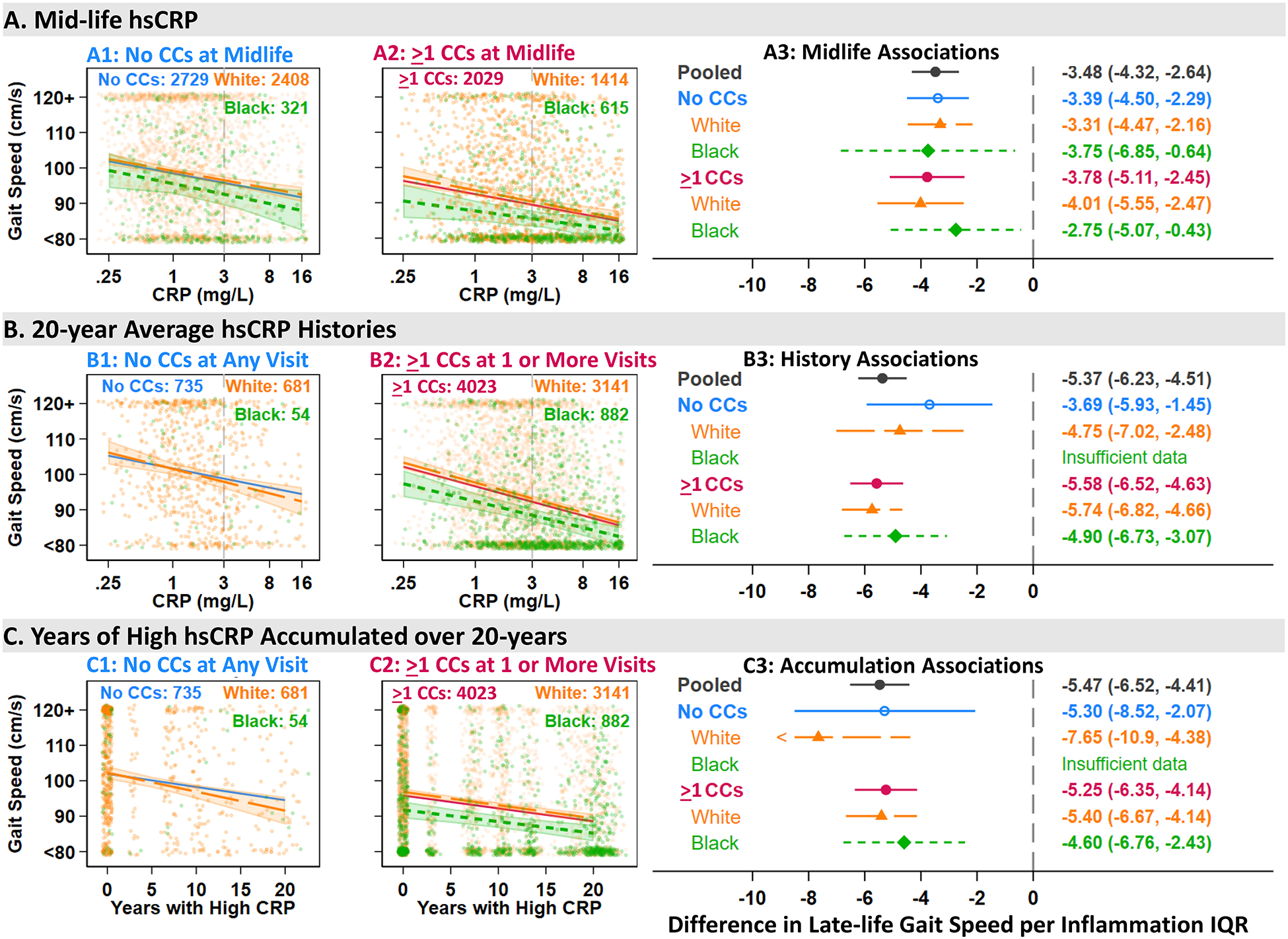
Results: High midlife hsCRP was associated with slower late-life gait speed, even among those without chronic conditions in midlife: -4.6 cm/s (95% CI: -6.4, -2.8). Importantly, sustained high hsCRP was associated with a 20-year slowing of -10.0 cm/s (-14.9, -5.1) among those who never experienced obesity, diabetes, or hypertension over the 20-year period. Associations were similar between Black participants, -3.8 cm/s (-6.9, -0.7) and White participants -3.3 (-4.5, -2.2) per interquartile range of midlife hsCRP; effect modifications by chronic conditions and race were unsupported throughout. Results were robust to accounting for SDoH or otherwise; however, worse SDoH was associated with higher inflammation and slower gait speed in both Black and White participants.
Conclusions: Inflammation in midlife may contribute to clinically meaningful late-life slowing of gait speed, even among otherwise healthy-appearing adults and regardless of race and socioeconomic disadvantage. Regular monitoring and interventions for inflammation may be warranted from midlife.
Keywords: chronic disease; gait speed; geriatrics functional assessment; inflammation; midlife; social determinants of health.
© 2024 The American Geriatrics Society.
Conflict of interest statement
Figures
Similar articles
-
Are Detailed, Patient-level Social Determinant of Health Factors Associated With Physical Function and Mental Health at Presentation Among New Patients With Orthopaedic Conditions?Clin Orthop Relat Res. 2023 May 1;481(5):912-921. doi: 10.1097/CORR.0000000000002446. Epub 2022 Oct 6. Clin Orthop Relat Res. 2023. PMID: 36201422 Free PMC article.
-
Limited association between multimorbidity and high-sensitive C-reactive protein or gait speed in community-dwelling octogenarians - findings from the BUTTERFLY study.J Nutr Health Aging. 2025 Jul;29(7):100603. doi: 10.1016/j.jnha.2025.100603. Epub 2025 Jun 16. J Nutr Health Aging. 2025. PMID: 40527275 Free PMC article.
-
Development, characterization, and replication of proteomic aging clocks: Analysis of 2 population-based cohorts.PLoS Med. 2024 Sep 24;21(9):e1004464. doi: 10.1371/journal.pmed.1004464. eCollection 2024 Sep. PLoS Med. 2024. PMID: 39316596 Free PMC article.
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
-
Multifaceted behavioral interventions to improve topical glaucoma therapy adherence in adults.Cochrane Database Syst Rev. 2025 Jun 11;6(6):CD015788. doi: 10.1002/14651858.CD015788.pub2. Cochrane Database Syst Rev. 2025. PMID: 40497459 Review.
References
MeSH terms
Substances
Grants and funding
- T35 AG038027/AG/NIA NIH HHS/United States
- U01 HL096812/HL/NHLBI NIH HHS/United States
- K24 HL152440/HL/NHLBI NIH HHS/United States
- U01 HL096917/HL/NHLBI NIH HHS/United States
- HHSN268201700004C/HB/NHLBI NIH HHS/United States
- AG054787/AG/NIA NIH HHS/United States
- U01 HL096902/HL/NHLBI NIH HHS/United States
- HHSN268201700001I/HL/NHLBI NIH HHS/United States
- U01 HL096899/HL/NHLBI NIH HHS/United States
- HHSN268201700003I/HL/NHLBI NIH HHS/United States
- National Institute on Aging Intramural Research Program
- Hearin Foundation, University of Mississippi Medical Center (UMMC) Medical Student Research Program
- HHSN268201700004I/HL/NHLBI NIH HHS/United States
- 5T35AG038027-06/AG/NIA NIH HHS/United States
- R01 AG054787/AG/NIA NIH HHS/United States
- U01 HL096814/HL/NHLBI NIH HHS/United States
- HHSN268201700005C/HL/NHLBI NIH HHS/United States
- HHSN268201700001C/HL/NHLBI NIH HHS/United States
- HHSN268201700002C/HB/NHLBI NIH HHS/United States
- HHSN268201700003C/HL/NHLBI NIH HHS/United States
- HHSN268201700002I/HL/NHLBI NIH HHS/United States
- HHSN268201700005I/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Research Materials
