Mortality rates among adult critical care patients with unusual or extreme values of vital signs and other physiological parameters: a retrospective study
- PMID: 38863361
- PMCID: PMC11167412
- DOI: 10.4266/acc.2023.01361
Mortality rates among adult critical care patients with unusual or extreme values of vital signs and other physiological parameters: a retrospective study
Abstract
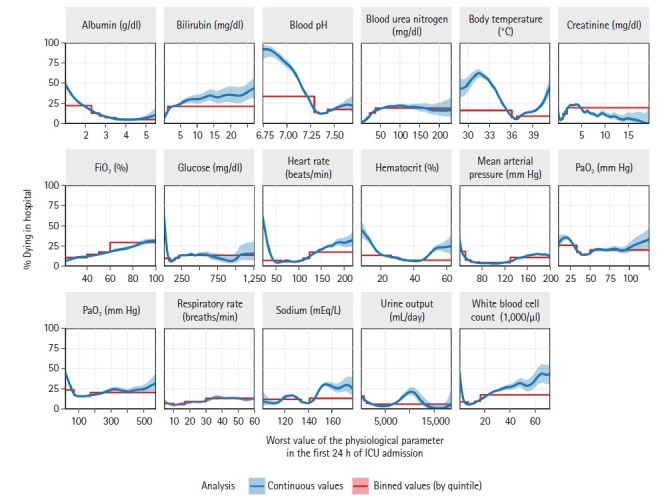
Background: We evaluated relationships of vital signs and laboratory-tested physiological parameters with in-hospital mortality, focusing on values that are unusual or extreme even in critical care settings.
Methods: We retrospectively studied Philips Healthcare-MIT eICU data (207 U.S. hospitals, 20142015), including 166,959 adult-patient critical care admissions. Analyzing most-deranged (worst) value measured in the first admission day, we investigated vital signs (body temperature, heart rate, mean arterial pressure, and respiratory rate) as well as albumin, bilirubin, blood pH via arterial blood gas (ABG), blood urea nitrogen, creatinine, FiO2 ABG, glucose, hematocrit, PaO2 ABG, PaCO2 ABG, sodium, 24-hour urine output, and white blood cell count (WBC).
Results: In-hospital mortality was ≥50% at extremes of low blood pH, low and high body temperature, low albumin, low glucose, and low heart rate. Near extremes of blood pH, temperature, glucose, heart rate, PaO2 , and WBC, relatively. Small changes in measured values correlated with several-fold mortality rate increases. However, high mortality rates and abrupt mortality increases were often hidden by the common practice of thresholding or binning physiological parameters. The best predictors of in-hospital mortality were blood pH, temperature, and FiO2 (scaled Brier scores: 0.084, 0.063, and 0.049, respectively).
Conclusions: In-hospital mortality is high and sharply increasing at extremes of blood pH, body temperature, and other parameters. Common-practice thresholding obscures these associations. In practice, vital signs are sometimes treated more casually than laboratory-tested parameters. Yet, vitals are easier to obtain and we found they are often the best mortality predictors, supporting perspectives that vitals are undervalued.
Keywords: acidosis; body temperature; fever; hypothermia; physiological parameters; vital signs.
Conflict of interest statement
Charles Harding received consulting fees from Exergen, including related to this report. Marybeth Pompei is Senior Vice President of Exergen and has thermometry patents. Dmitriy Burmistrov reports no conflicts of interest. Francesco Pompei is CEO of Exergen and has thermometry patents. Exergen, Corp. is a manufacturer of thermometers. No other potential conflicts of interest relevant to this article were reported.
Figures
Similar articles
-
[Risk factors analysis of acute respiratory distress syndrome in intensive care unit traumatic patients].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2018 Oct;30(10):978-982. doi: 10.3760/cma.j.issn.2095-4352.2018.010.015. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2018. PMID: 30439321 Chinese.
-
The prevalence and diagnostic utility of systemic inflammatory response syndrome vital signs in a pediatric emergency department.Acad Emerg Med. 2015 Apr;22(4):381-9. doi: 10.1111/acem.12610. Epub 2015 Mar 16. Acad Emerg Med. 2015. PMID: 25778743
-
[Improvement effect of early goal-directed therapy on the prognosis in patients with septic shock].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2015 Nov;27(11):899-905. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2015. PMID: 27132457 Chinese.
-
Distribution of Extreme Vital Signs and Complete Blood Count Values of Healthy Parturients: A Retrospective Database Analysis and Review of the Literature.Anesth Analg. 2019 Dec;129(6):1595-1606. doi: 10.1213/ANE.0000000000003866. Anesth Analg. 2019. PMID: 31743180 Review.
-
Artificial intelligence in clinical care amidst COVID-19 pandemic: A systematic review.Comput Struct Biotechnol J. 2021;19:2833-2850. doi: 10.1016/j.csbj.2021.05.010. Epub 2021 May 7. Comput Struct Biotechnol J. 2021. PMID: 34025952 Free PMC article. Review.
Cited by
-
Association between a high Modified Nutrition Risk in Critically Ill score and 30-day mortality in critically ill adults: A retrospective cohort study.Ir J Med Sci. 2025 Aug 14. doi: 10.1007/s11845-025-04066-4. Online ahead of print. Ir J Med Sci. 2025. PMID: 40810829
References
-
- Knaus WA, Wagner DP, Draper EA, Zimmerman JE, Bergner M, Bastos PG, et al. The APACHE III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest. 1991;100:1619–36. - PubMed
-
- Zimmerman JE, Kramer AA, McNair DS, Malila FM. Acute Physiology and Chronic Health Evaluation (APACHE) IV: hospital mortality assessment for today's critically ill patients. Crit Care Med. 2006;34:1297–310. - PubMed
-
- Higgins TL, Teres D, Copes WS, Nathanson BH, Stark M, Kramer AA. Assessing contemporary intensive care unit outcome: an updated Mortality Probability Admission Model (MPM0-III) Crit Care Med. 2007;35:827–35. - PubMed
LinkOut - more resources
Full Text Sources