

Outcome of Cerebral Aneurysm Clipping in Nigeria: A Single-Centre Experience
- PMID: 38863464
- PMCID: PMC11163260
- DOI: 10.60787/NMJ-63-4-75
Outcome of Cerebral Aneurysm Clipping in Nigeria: A Single-Centre Experience
Abstract
Background: Ruptured cerebral artery aneurysms (RCAA) are devastating diseases with high morbidity and mortality rates if not promptly managed. In Nigeria, access to timely neurosurgical services remains a challenge and aneurysm coiling is still not possible in virtually all centres in Nigeria. The aim of this study is to report on our 9 years' experience with clipping of cerebral aneurysm and on the attendant clinical outcomes.
Methodology: A retrospective analysis of all consecutive operated RCAA between March 2012 and June 2021 was conducted. Patients' demographic parameters, World Federation of Neurosurgical Societies (WFNS) grade, Hunt and Hess (HH) grade, aneurysm location, timing of surgery and outcome were analysed. Outcome was measured using Glasgow Outcome Scale (GOS) score.
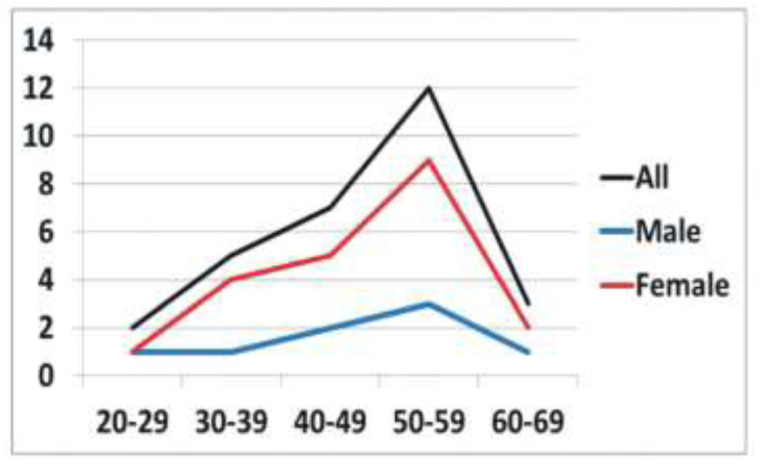
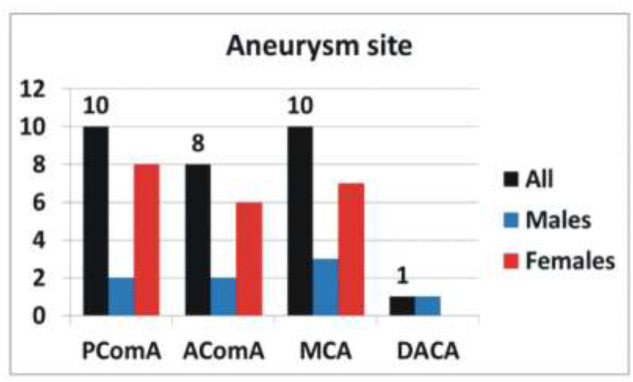
Results: A total 29 were included in the study. The most common age group affected was between 50-59 years. RCAA were mainly in the region of the middle cerebral artery and posterior communicating artery (PComA) territories. All the patients presented after 24 hours of the ictus. Two (6.9%) patients had multiple aneurysms. Early clipping (<72hours after presentation) was possible in 8 (27.6%) patients. At least one episode of a rebleed occurred in 19 (65.5%) patients prior to surgery. Mortality rate was 17.2%. None of the patients with PComA aneurysm died. The patients' pre-operative WFNS and HH grades were significantly associated with GOS.
Conclusion: Modifiable factors like under diagnoses, delayed referral, cultural belief and financial challenges may account for the low number of patients presenting for neurosurgical care. The possibility of a sizeable number of patients dying due to these factors is a strong possibility for the low number of patients presenting for neurosurgical care.
Keywords: Aneurysm; Anterior Communicating Artery; Clipping; Middle Cerebral Artery; Posterior Communicating Artery.
Copyright © 2022 Nigerian Medical Association.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
The Factors Associated with Outcomes in Surgically Managed Ruptured Cerebral Aneurysm.Malays J Med Sci. 2018 Feb;25(1):32-41. doi: 10.21315/mjms2018.25.1.5. Epub 2018 Feb 28. Malays J Med Sci. 2018. PMID: 29599633 Free PMC article.
-
Outcomes for clip ligation and hematoma evacuation associated with 102 patients with ruptured middle cerebral artery aneurysms.World Neurosurg. 2013 Sep-Oct;80(3-4):335-41. doi: 10.1016/j.wneu.2012.03.008. Epub 2012 Mar 30. World Neurosurg. 2013. PMID: 22465372
-
Endovascular coiling versus neurosurgical clipping for people with aneurysmal subarachnoid haemorrhage.Cochrane Database Syst Rev. 2018 Aug 15;8(8):CD003085. doi: 10.1002/14651858.CD003085.pub3. Cochrane Database Syst Rev. 2018. PMID: 30110521 Free PMC article.
-
Endoscope-assisted microneurosurgery for anterior circulation aneurysms using the angle-type rigid endoscope over a 3-year period.Childs Nerv Syst. 2004 Nov;20(11-12):811-5. doi: 10.1007/s00381-004-0935-1. Epub 2004 Jun 23. Childs Nerv Syst. 2004. PMID: 15221249 Clinical Trial.
-
Neuropsychological function after endovascular and neurosurgical treatment of subarachnoid hemorrhage: a systematic review and meta-analysis.J Neurosurg. 2018 Mar;128(3):768-776. doi: 10.3171/2016.11.JNS162055. Epub 2017 Apr 14. J Neurosurg. 2018. PMID: 28409729
Cited by
-
Surgical outcomes of delayed clipping in ruptured intracranial aneurysms of anterior circulation: Experience from a low-middle-income country.Pak J Med Sci. 2024 Dec;40(12PINS Suppl):S41-S46. doi: 10.12669/pjms.40.12(PINS).11273. Pak J Med Sci. 2024. PMID: 39703957 Free PMC article.
References
-
- Vlak MH, Algra A, Brandenburg R, Rinkel GJ. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: a systematic review and meta-analysis. Lancet Neurol. 2011;10:626–36. - PubMed
-
- Udy AA, Schweikert S, Anstey J, Anstey M, Cohen J, Flower O, Saxby E, Poll AV, Delaney A. Critical care management of aneurysmal subarachnoid haemorrhage in Australia and New Zealand: what are we doing, and where to from here? Crit Care Resusc. 2017; 19:103–9. - PubMed
-
- Wiebers DO, Whisnant JP, Huston J III, Meissner I, Brown RD Jr, Piepgras DR. Unruptured intracranial aneurysms: Natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet. 2003;362:103–10. - PubMed
LinkOut - more resources
Full Text Sources