

The Effect of Greater Area Deprivation and Medicaid Insurance Status on Timing of Care and Rate of Reinjury After Anterior Cruciate Ligament Reconstruction
- PMID: 38863506
- PMCID: PMC11165962
- DOI: 10.1177/23259671241240751
The Effect of Greater Area Deprivation and Medicaid Insurance Status on Timing of Care and Rate of Reinjury After Anterior Cruciate Ligament Reconstruction
Abstract
Background: Lower socioeconomic status and public insurance lead to a longer delay to surgery and a higher likelihood of concomitant pathology before undergoing anterior cruciate ligament reconstruction (ACLR). However, few studies have examined the influence of community deprivation on ACLR timing and outcomes.
Purpose/hypothesis: The primary aim of this study was to define the effect of the area deprivation index (ADI) and insurance classification on access to orthopaedic care after an ACL rupture, and the secondary aim was to determine whether these variables were associated with a second ACL injury after primary ACLR. It was hypothesized that patients with a greater national ADI percentile and Medicaid insurance would experience longer delays to care and an increased risk of reinjury after ACLR.
Study design: Cohort study; Level of evidence, 3.
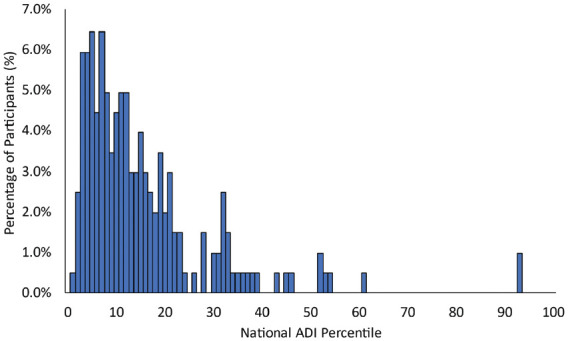
Methods: A retrospective study was performed to evaluate patients undergoing primary ACLR between 2016 and 2019. The national ADI percentile was obtained utilizing the Neighborhood Atlas website. The relationship between national ADI percentile and care characteristics (eg, time to specialized care) was investigated using the Spearman rho correlation coefficient (r). The association between patient and care characteristics and second ACL injury after the index procedure (ie, graft rerupture or contralateral ACL rupture) was investigated using binary logistic regression.
Results: A total of 197 patients met the inclusion criteria. Longer times from injury to surgery (r = 0.238; P < .001) and from specialized care to surgery (r = 0.217; P = .002) were associated with a greater national ADI percentile. The second injury group reported significantly greater national ADI (P = .026) and included a greater percentage of patients with Medicaid insurance (31.3%) compared with the no second injury group. Patients experienced 5.1% greater odds of a second ACL injury for each additional month between evaluation and surgery.
Conclusion: Greater national ADI percentile and Medicaid insurance status were associated with adverse ACLR timing and outcomes. Patients with a greater national ADI percentile took significantly longer to obtain surgery after ACL injury. Those who sustained a second ACL injury after ACLR had an overall higher mean national ADI percentile and included a greater proportion of patients with Medicaid compared with those who did not sustain a second ACL injury. Future studies should critically investigate the underlying factors of these associations to reach equity in orthopaedic care.
Keywords: anterior cruciate ligament; area deprivation index; general; knee; ligaments; socioeconomic status.
© The Author(s) 2024.
Conflict of interest statement
The authors declared that they have the following conflicts of interest: A.J.C. has received education payments from Arthrex, Medwest Associates, Mid-Atlantic Surgical Systems LLC, Smith+Nephew, and Supreme Orthopedic Systems LLC; hospitality payments from Stryker; and a grant from Arthrex. B.M.B. has received education payments from Conetic Solutions, Arthrex, Smith+Nephew, and Medwest Associates; hospitality payments from Stryker, Smith+Nephew, Conetic Solutions, and Medical Device Business Services; honoraria from Encore Medical LP; and a grant from Arthrex. C.M.C. has received education payments from Liberty Surgical and hospitality payments from Medical Device Business Services. E.S.C. has received consulting fees from Avanos Medical; education payments from Arthrex and Supreme Orthopedic Systems LLC; and hospitality payments from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. Ethical approval for this study was obtained from the Western Institutional Review Board-Copernicus Group (ref No. 20216925).
Figures
Similar articles
-
Factors Influencing Return to Play and Second Anterior Cruciate Ligament Injury Rates in Level 1 Athletes After Primary Anterior Cruciate Ligament Reconstruction: 2-Year Follow-up on 1432 Reconstructions at a Single Center.Am J Sports Med. 2020 Mar;48(4):812-824. doi: 10.1177/0363546519900170. Epub 2020 Feb 7. Am J Sports Med. 2020. PMID: 32031870 Free PMC article.
-
Fear of Reinjury Following Surgical and Nonsurgical Management of Anterior Cruciate Ligament Injury: An Exploratory Analysis of the NACOX Multicenter Longitudinal Cohort Study.Phys Ther. 2022 Feb 1;102(2):pzab273. doi: 10.1093/ptj/pzab273. Phys Ther. 2022. PMID: 34939109 Free PMC article. Clinical Trial.
-
Predicting Anterior Cruciate Ligament Reinjury From Return-to-Activity Assessments at 6 Months Postsurgery: A Prospective Cohort Study.J Athl Train. 2022 Apr 1;57(4):325-333. doi: 10.4085/1062-6050-0407.20. J Athl Train. 2022. PMID: 35439312 Free PMC article.
-
Early Operative Versus Delayed or Nonoperative Treatment of Anterior Cruciate Ligament Injuries in Pediatric Patients.J Athl Train. 2016 May;51(5):425-7. doi: 10.4085/1062-6050.51.5.11. Epub 2016 May 31. J Athl Train. 2016. PMID: 27244126 Free PMC article. Review.
-
Passive anterior tibia translation in anterior cruciate ligament-injured, anterior cruciate ligament-reconstructed and healthy knees: a systematic review.Musculoskelet Surg. 2019 Aug;103(2):121-130. doi: 10.1007/s12306-018-0572-6. Epub 2018 Oct 16. Musculoskelet Surg. 2019. PMID: 30328030 Free PMC article.
Cited by
-
The Forward Movement: Amplifying Black Voices on Race and Orthopaedics-We Must Understand the Value of Health Equity.Clin Orthop Relat Res. 2024 Oct 1;482(10):1768-1769. doi: 10.1097/CORR.0000000000003238. Epub 2024 Sep 12. Clin Orthop Relat Res. 2024. PMID: 39321352 No abstract available.
References
-
- Brambilla L, Pulici L, Carimati G, et al.. Prevalence of associated lesions in anterior cruciate ligament reconstruction: correlation with surgical timing and with patient age, sex, and body mass index. Am J Sports Med. 2015;43(12):2966-2973. - PubMed
-
- Chava NS, Fortier LM, Verma N, et al.. Patients with Medicaid insurance undergoing anterior cruciate ligament reconstruction have lower postoperative International Knee Documentation Committee scores and are less likely to return to sport than privately insured patients. Arthrosc Sports Med Rehabil. 2022;4(4):e1457-e1464. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
