

Three-year follow-up study reveals improved survival rate in NSCLC patients underwent guideline-concordant diagnosis and treatment
- PMID: 38863625
- PMCID: PMC11165022
- DOI: 10.3389/fonc.2024.1382197
Three-year follow-up study reveals improved survival rate in NSCLC patients underwent guideline-concordant diagnosis and treatment
Abstract
Background: No studies in China have assessed the guideline-concordance level of the first-course of non-small cell lung cancer (NSCLC) diagnosis and treatment and its relationship with survival. This study comprehensively assesses the current status of guideline-concordant diagnosis (GCD) and guideline-concordant treatment (GCT) of NSCLC in China and explores its impact on survival.
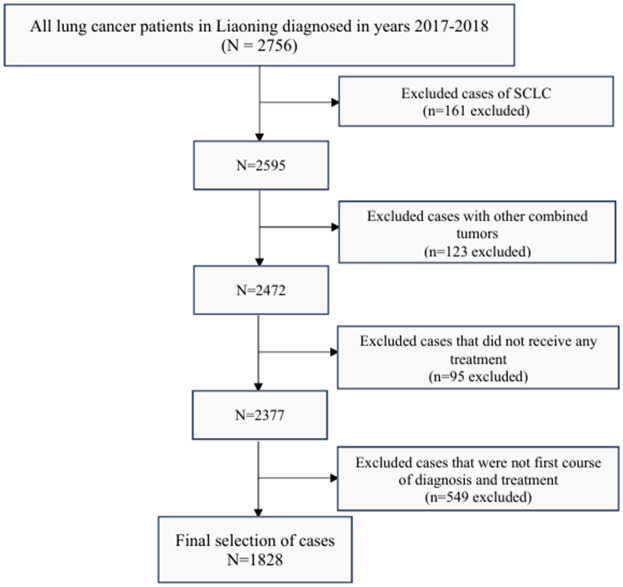
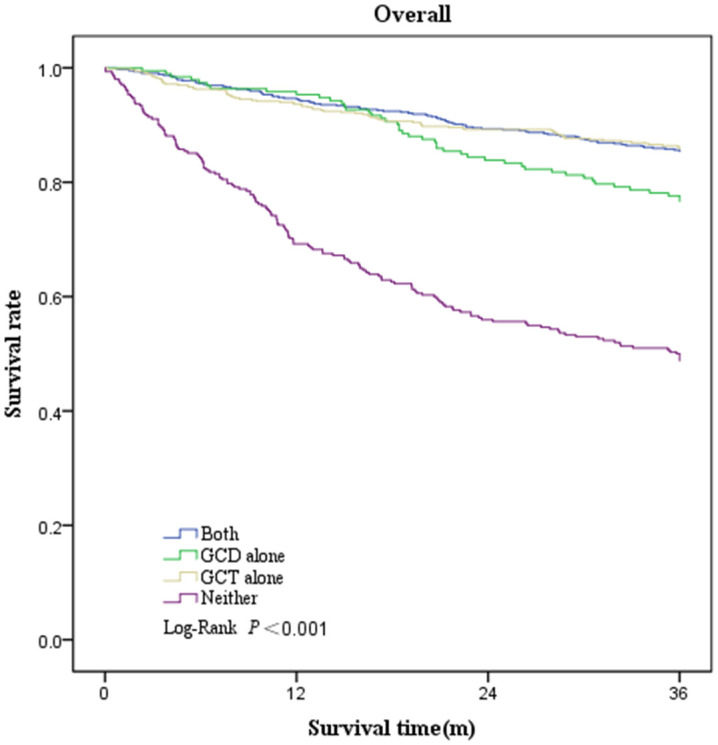
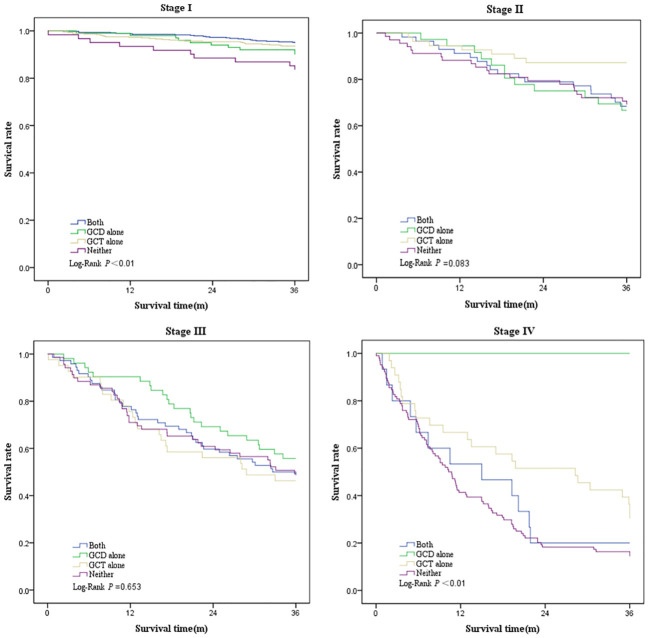
Methods: First course diagnosis and treatment data for NSCLC patients in Liaoning, China in 2017 and 2018 (n=1828) were used and classified by whether they underwent GCD and GCT according to Chinese Society of Clinical Oncology (CSCO) guidelines. Pearson's chi-squared test was used to determine unadjusted associations between categorical variables of interest. Logistic models were constructed to identify variables associated with GCD and GCT. Kaplan-Meier analysis and log-rank tests were used to estimate and compare 3-year survival rates. Multivariate Cox proportional risk models were constructed to assess the risk of cancer mortality associated with guideline-concordant diagnosis and treatment.
Results: Of the 1828 patients we studied, 48.1% underwent GCD, and 70.1% underwent GCT. The proportions of patients who underwent both GCD and GCT, GCD alone, GCT alone and neither GCD nor GCT were 36.7%, 11.4%, 33.5% and 18.4%, respectively. Patients in advanced stage and non-oncology hospitals were significantly less likely to undergo GCD and GCT. Compared with those who underwent neither GCD nor GCT, patients who underwent both GCD and GCT, GCD alone and GCT alone had 35.2%, 26.7% and 35.7% higher 3-year survival rates; the adjusted lung cancer mortality risk significantly decreased by 29% (adjusted hazard ratio[aHR], 0.71; 95% CI, 0.53-0.95), 29% (aHR, 0.71; 95% CI, 0.50-1.00) and 32% (aHR, 0.68; 95% CI, 0.51-0.90).
Conclusion: The 3-year risk of death is expected to be reduced by 29% if patients with NSCLC undergo both GCD and GCT. There is a need to establish an oncology diagnosis and treatment data management platform in China to monitor, evaluate, and promote the use of clinical practice guidelines in healthcare settings.
Keywords: diagnosis and treatment; first course; guideline-concordant; lung cancer; survival.
Copyright © 2024 Mu, Yang, Li, Zhou, Liu, Zhang, Wang, Chen, Yan, Sun and Pan.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Stage-Specific Guideline Concordant Treatment Impacts on Survival in Nonsmall Cell Lung Cancer: A Novel Quality Indicator.Clin Lung Cancer. 2024 Dec;25(8):e466-e478. doi: 10.1016/j.cllc.2024.08.012. Epub 2024 Aug 24. Clin Lung Cancer. 2024. PMID: 39304361
-
National trends and survival outcomes associated with non-guideline-concordant treatment of inflammatory breast cancer.Breast Cancer Res Treat. 2025 Jun;211(2):527-535. doi: 10.1007/s10549-025-07669-8. Epub 2025 Mar 18. Breast Cancer Res Treat. 2025. PMID: 40100496 Free PMC article.
-
The Relative Survival Impact of Guideline-Concordant Clinical Staging and Stage-Appropriate Treatment of Potentially Curable Non-Small Cell Lung Cancer.Chest. 2022 Jul;162(1):242-255. doi: 10.1016/j.chest.2022.01.046. Epub 2022 Feb 3. Chest. 2022. PMID: 35122751
-
Guideline-concordant timely lung cancer care and prognosis among elderly patients in the United States: A population-based study.Cancer Epidemiol. 2015 Dec;39(6):1136-44. doi: 10.1016/j.canep.2015.06.005. Epub 2015 Jun 29. Cancer Epidemiol. 2015. PMID: 26138902 Free PMC article.
-
Guideline-concordant lung cancer care and associated health outcomes among elderly patients in the United States.J Geriatr Oncol. 2015 Mar;6(2):101-10. doi: 10.1016/j.jgo.2015.01.001. Epub 2015 Jan 17. J Geriatr Oncol. 2015. PMID: 25604094 Free PMC article.
Cited by
-
The Saudi Thoracic Society Evidence-based guidelines for the diagnosis and management of chronic obstructive pulmonary disease.Ann Thorac Med. 2025 Jan-Mar;20(1):1-35. doi: 10.4103/atm.atm_155_24. Epub 2024 Sep 24. Ann Thorac Med. 2025. PMID: 39926399 Free PMC article.
References
-
- Allemani C, Matsuda T, Di Carlo V, Harewood R, Matz M, Nikšić M, et al. . Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet. (2018) 391:1023–75. doi: 10.1016/S0140-6736(17)33326-3 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources