

Long-term safety and impact of immune recovery in heavily treatment-experienced adults receiving fostemsavir for up to 5 years in the phase 3 BRIGHTE study
- PMID: 38863717
- PMCID: PMC11165140
- DOI: 10.3389/fimmu.2024.1394644
Long-term safety and impact of immune recovery in heavily treatment-experienced adults receiving fostemsavir for up to 5 years in the phase 3 BRIGHTE study
Abstract
Introduction: Fostemsavir is a gp120-directed attachment inhibitor approved for heavily treatment-experienced (HTE) adults with multidrug-resistant HIV-1. We provide detailed week 240 safety results from the BRIGHTE study and evaluate the impact of immune recovery on safety outcomes.
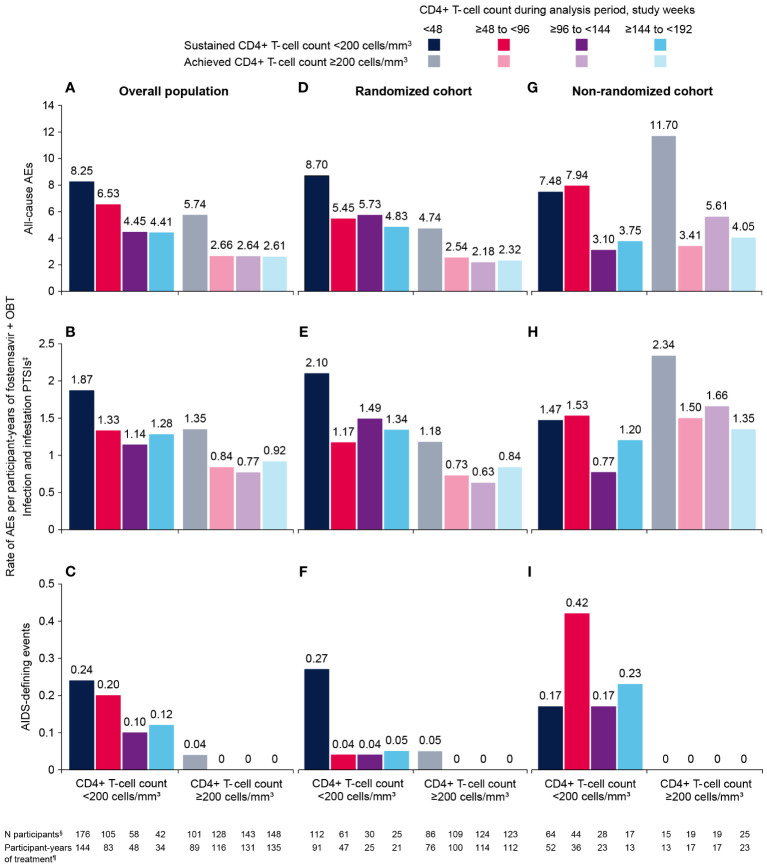
Methods: The phase 3 BRIGHTE trial is ongoing; data for this analysis were collected from the first participant's first visit (February 23, 2015) through the last participant's last visit for week 240 (March 22, 2021). Safety endpoints were assessed in participants who received fostemsavir + optimized background therapy. In participants with baseline CD4+ T-cell count <200 cells/mm3, exposure-adjusted adverse event (AE) rates were assessed among subgroups with or without CD4+ T-cell count ≥200 cells/mm3 at any time during 48-week analysis periods through week 192.
Results: Through a median of 258 weeks (range, 0.14-319) of treatment, discontinuations due to AEs occurred in 30/371 (8%) participants. Serious AEs were reported in 177/371 (48%) participants, including 16 drug-related events in 13 (4%) participants. Thirty-five (9%) deaths occurred, primarily related to AIDS or acute infections. COVID-19-related events occurred in 25 (7%) participants; all resolved without sequelae. Among participants with baseline CD4+ T-cell count <200 cells/mm3, 122/162 (75%) achieved CD4+ T-cell count ≥200 cells/mm3 at week 192. Exposure-adjusted AE rates were markedly lower among participants achieving CD4+ T-cell count ≥200 cells/mm3 at any time vs those sustaining <200 cells/mm3. No new AIDS-defining events were reported after week 48 in participants with CD4+ T-cell count ≥200 cells/mm3.
Conclusions: Cumulative safety findings through the BRIGHTE 240-week interim analysis are consistent with other trials in HTE participants with advanced HIV-1 and comorbid disease. Reduced rates of AIDS-defining events and AEs were observed in participants with immunologic recovery on fostemsavir-based treatment.
Clinical trial number: NCT02362503, https://clinicaltrials.gov/study/NCT02362503.
Keywords: ARV; clinical trials; drug resistance; intervention; treatment.
Copyright © 2024 Llibre, Aberg, Walmsley, Velez, Zala, Crabtree Ramírez, Shepherd, Shah, Clark, Tenorio, Pierce, Du, Li, Wang, Chabria and Warwick-Sanders.
Conflict of interest statement
JL has participated in scientific advisory boards for Gilead, Janssen-Cilag, and ViiV Healthcare. JA has received grants from Emergent BioSolutions, Frontier Technologies, Gilead, GSK, Janssen, Merck, Pfizer, Regeneron, and ViiV Healthcare, which were paid to her institution, and has participated in scientific advisory boards for GSK, Merck, and ViiV Healthcare. SW has received investigator-initiated grants from Gilead, Merck, and ViiV Healthcare and has participated in advisory boards for Merck and ViiV Healthcare. CZ has received grants from GSK. BCR has participated in advisory boards for Gilead, GSK, and ViiV Healthcare, and her institution has received grants for conducting clinical trials from Janssen and MSD. BS, RS, AC, AT, AP, FD, BL, MW, and MW-S are employees of GSK or ViiV Healthcare and may own stock in GSK. SC was an employee of ViiV Healthcare at the time of the study and may own stock in GSK. The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Safety and efficacy of the HIV-1 attachment inhibitor prodrug fostemsavir in heavily treatment-experienced individuals: week 96 results of the phase 3 BRIGHTE study.Lancet HIV. 2020 Nov;7(11):e740-e751. doi: 10.1016/S2352-3018(20)30240-X. Lancet HIV. 2020. PMID: 33128903 Clinical Trial.
-
Comparative Efficacy and Safety of Fostemsavir in Heavily Treatment-Experienced People With HIV-1.Clin Ther. 2022 Jun;44(6):886-900. doi: 10.1016/j.clinthera.2022.04.007. Epub 2022 May 21. Clin Ther. 2022. PMID: 35610081
-
Long-term efficacy and safety of fostemsavir among subgroups of heavily treatment-experienced adults with HIV-1.AIDS. 2021 Jun 1;35(7):1061-1072. doi: 10.1097/QAD.0000000000002851. AIDS. 2021. PMID: 33946085 Free PMC article.
-
Week 240 Efficacy and Safety of Fostemsavir Plus Optimized Background Therapy in Heavily Treatment-Experienced Adults with HIV-1.Infect Dis Ther. 2023 Sep;12(9):2321-2335. doi: 10.1007/s40121-023-00870-6. Epub 2023 Sep 26. Infect Dis Ther. 2023. PMID: 37751019 Free PMC article.
-
Fostemsavir for the treatment of HIV.Expert Rev Anti Infect Ther. 2021 Aug;19(8):961-966. doi: 10.1080/14787210.2021.1865801. Epub 2021 Jan 4. Expert Rev Anti Infect Ther. 2021. PMID: 33331202 Review.
Cited by
-
Inflammatory Biomarker Reduction With Fostemsavir Over 96 Weeks in Heavily Treatment-Experienced Adults With Multidrug-Resistant HIV-1 in the BRIGHTE Study.Open Forum Infect Dis. 2024 Aug 26;11(9):ofae469. doi: 10.1093/ofid/ofae469. eCollection 2024 Sep. Open Forum Infect Dis. 2024. PMID: 39233711 Free PMC article. Clinical Trial.
References
-
- Pelchen-Matthews A, Borges ÁH, Reekie J, Rasmussen LD, Wiese L, Weber J, et al. . Prevalence and outcomes for heavily treatment-experienced individuals living with human immunodeficiency virus in a European cohort. J Acquir Immune Defic Syndr. (2021) 87:806–17. doi: 10.1097/QAI.0000000000002635 - DOI - PubMed
-
- Rukobia. [prescribing information]. Durham, NC: ViiV Healthcare; (2024).
-
- Trogarzo. [prescribing information]. Montréal, Canada: Theratechnologies Inc; (2023).
-
- Sunlenca. [prescribing information]. Foster City, CA: Gilead Sciences, Inc; (2022).
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials