

Recommended dosages of analgesic and sedative drugs in intensive care result in a low incidence of potentially toxic blood concentrations
- PMID: 38863729
- PMCID: PMC11165249
- DOI: 10.48101/ujms.v129.10560
Recommended dosages of analgesic and sedative drugs in intensive care result in a low incidence of potentially toxic blood concentrations
Abstract
Background: Standard dosages of analgesic and sedative drugs are given to intensive care patients. The resulting range of blood concentrations and corresponding clinical responses need to be better examined. The purpose of this study was to describe daily dosages, measured blood concentrations, and clinical responses in critically ill patients. The purpose was also to contribute to establishing whole blood concentration reference values of the drugs investigated.
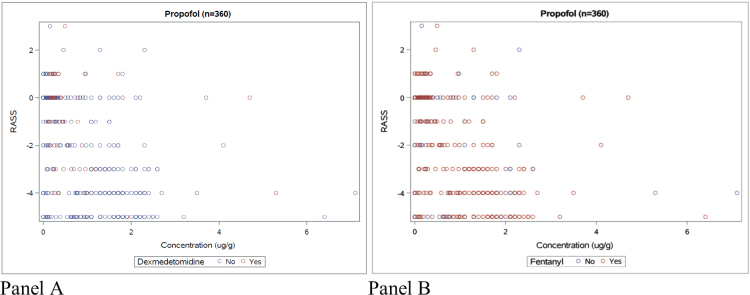
Methods: A descriptive study of prospectively collected data from 302 admissions to a general intensive care unit (ICU) at a university hospital. Ten drugs (clonidine, fentanyl, morphine, dexmedetomidine, ketamine, ketobemidone, midazolam, paracetamol, propofol, and thiopental) were investigated, and daily dosages recorded. Blood samples were collected twice daily, and drug concentrations were measured. Clinical responses were registered using Richmond agitation-sedation scale (RASS) and Numeric rating scale (NRS).
Results: Drug dosages were within recommended dose ranges. Blood concentrations for all 10 drugs showed a wide variation within the cohort, but only 3% were above therapeutic interval where clonidine (57 of 122) and midazolam (38 of 122) dominated. RASS and NRS were not correlated to drug concentrations.
Conclusion: Using recommended dose intervals for analgesic and sedative drugs in the ICU setting combined with regular monitoring of clinical responses such as RASS and NRS leads to 97% of concentrations being below the upper limit in the therapeutic interval. This study contributes to whole blood drug concentration reference values regarding these 10 drugs.
Keywords: Analgesia; critical care; drug concentrations; drug dosages; intensive care medicine; sedation.
© 2024 The Author(s).
Conflict of interest statement
The authors report no conflict of interest.
Figures



Similar articles
-
Comparison of pre-mortem and post-mortem blood concentrations of analgesic and sedative drugs in intensive care patients.Forensic Sci Int. 2025 Oct;375:112551. doi: 10.1016/j.forsciint.2025.112551. Epub 2025 Jul 4. Forensic Sci Int. 2025. PMID: 40638968
-
Clinical sedation scores as indicators of sedative and analgesic drug exposure in intensive care unit patients.Am J Geriatr Pharmacother. 2007 Sep;5(3):218-31. doi: 10.1016/j.amjopharm.2007.10.005. Am J Geriatr Pharmacother. 2007. PMID: 17996661
-
Altered Pharmacokinetics in Prolonged Infusions of Sedatives and Analgesics Among Adult Critically Ill Patients: A Systematic Review.Clin Ther. 2018 Sep;40(9):1598-1615.e2. doi: 10.1016/j.clinthera.2018.07.021. Epub 2018 Aug 31. Clin Ther. 2018. PMID: 30173953
-
Concentrations of remifentanil, propofol, fentanyl, and midazolam during rewarming from therapeutic hypothermia.Acta Anaesthesiol Scand. 2014 Jul;58(6):709-15. doi: 10.1111/aas.12300. Epub 2014 Mar 11. Acta Anaesthesiol Scand. 2014. PMID: 24611449
-
[Agents for sedation and analgesia in the intensive care unit].Ann Fr Anesth Reanim. 2008 Jul-Aug;27(7-8):560-6. doi: 10.1016/j.annfar.2008.04.008. Epub 2008 Jul 1. Ann Fr Anesth Reanim. 2008. PMID: 18595650 French.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources