

Efficiency of polymyxin B treatment against nosocomial infection: a systematic review and meta-analysis
- PMID: 38863886
- PMCID: PMC11165566
- DOI: 10.3389/fmed.2024.1400757
Efficiency of polymyxin B treatment against nosocomial infection: a systematic review and meta-analysis
Abstract
Background: Some cohort studies have explored the effects and safety of polymyxin B (PMB) in comparison to other antibiotics for the treatment of nosocomial infections, yielding inconsistent results. This systematic review aims to explore the effectiveness and safety of PMB and compared it with other antibiotics.
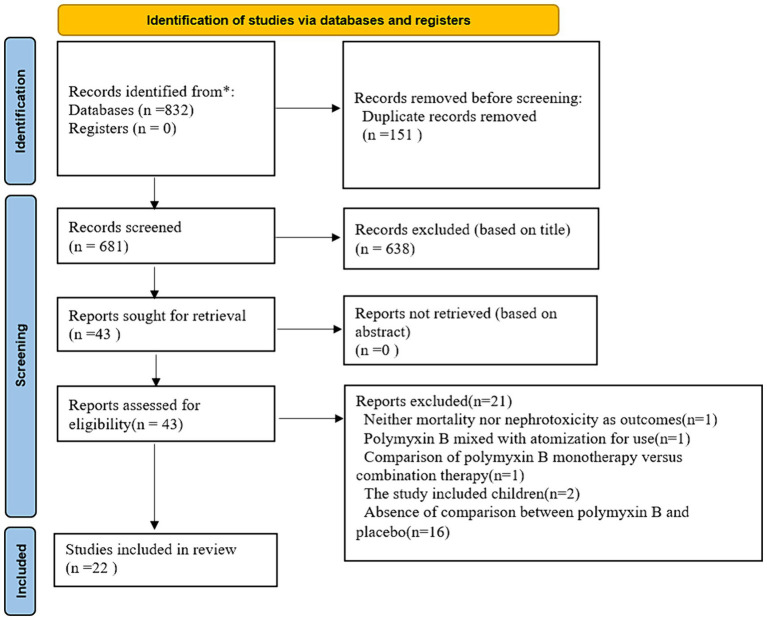
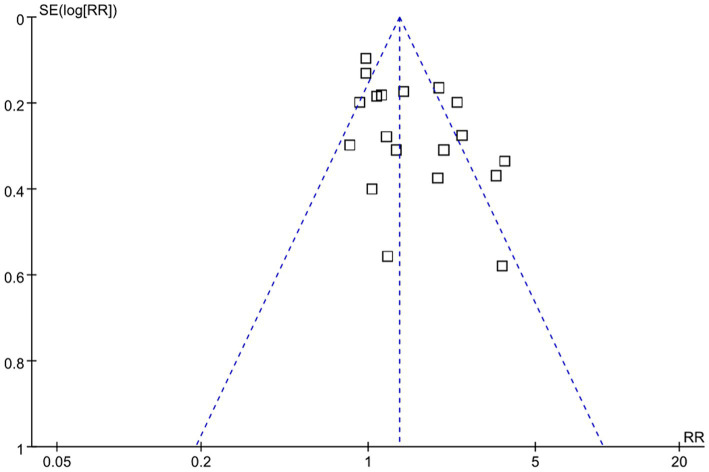
Methods: A systematic literature search was conducted in PubMed, Embase, the Cochrane Library, and Web of Science, searching specific terms to identify quantitative cohort studies or RCTs that compared the effects of PMB with other antibiotics in terms of their efficacy and safety. The Newcastle-Ottawa Scale (NOS) was conducted to evaluate the risk of bias of observational studies. Odds ratios with 95% confidence intervals were used for outcome assessment. We evaluated heterogeneity using the I 2 test.
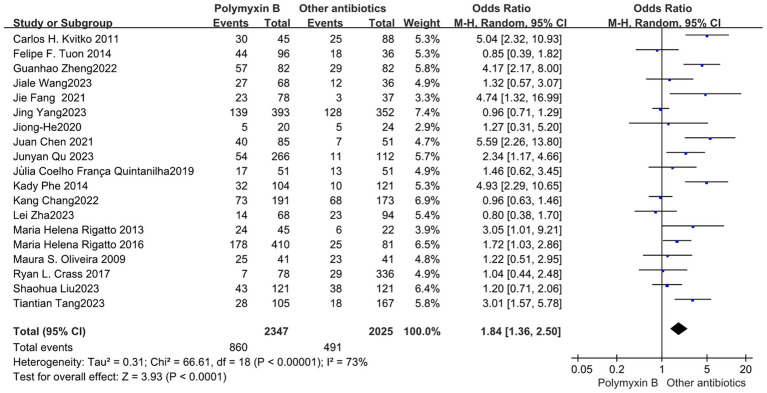
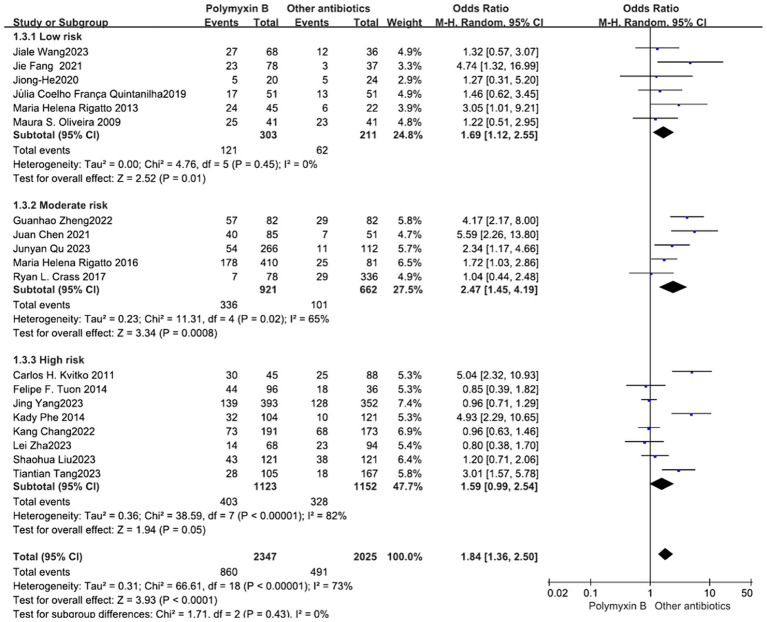
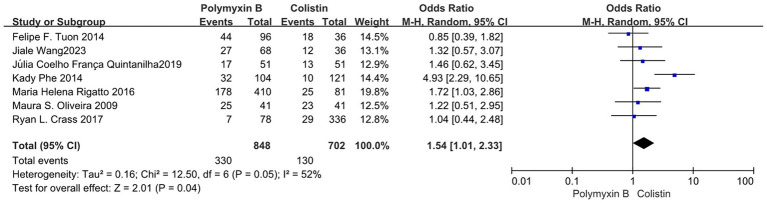
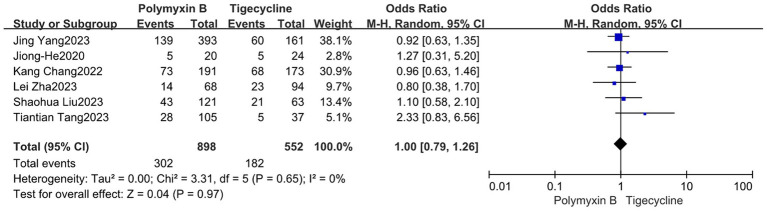
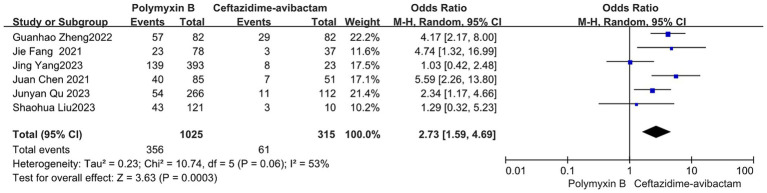
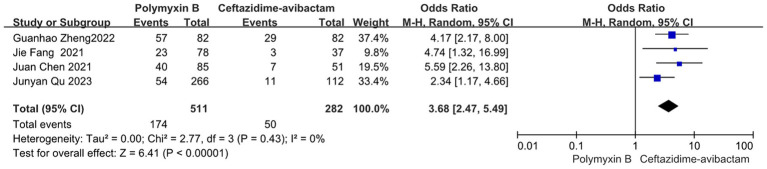
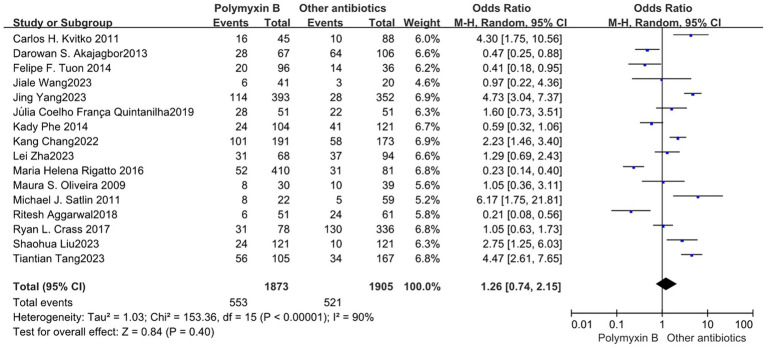
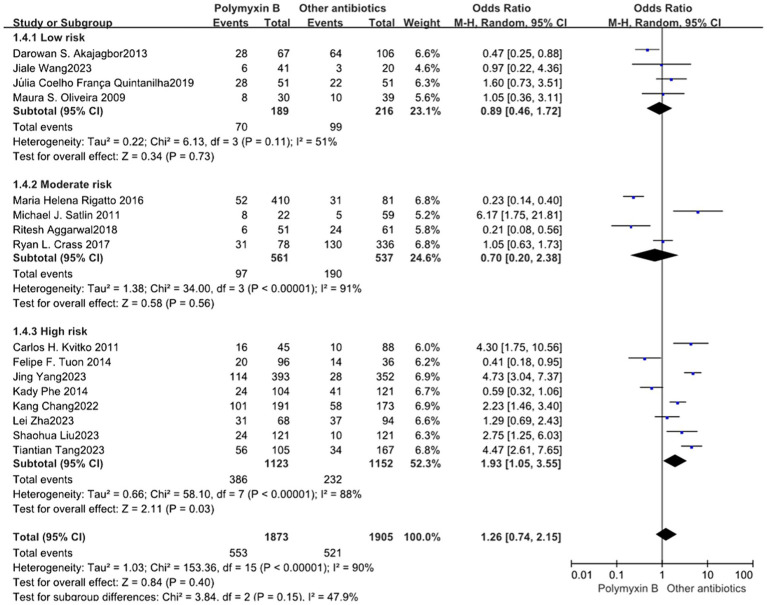
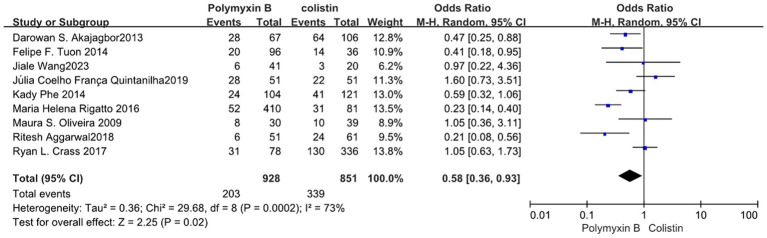
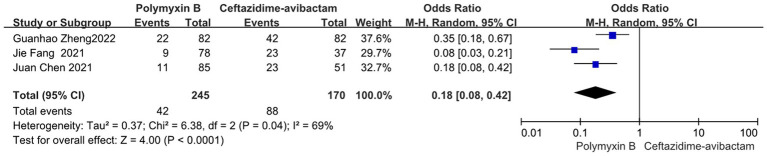
Results: A total of 22 observational trials were included in the analysis. The PMB group had a higher mortality rate compared to the control group (odds ratio: 1.84, 95% CI: 1.36-2.50, p<0.00001, I 2 = 73%). while, the ceftazidime-avibactam group demonstrated a distinct advantage with lower mortality rates, despite still exhibiting high heterogeneity (odds ratio 2.73, 95% confidence interval 1.59-4.69; p = 0.0003; I 2 = 53%). Additionally, the PMB group had a lower nephrotoxicity rate compared to the colistin group but exhibited high heterogeneity in the results (odds ratio 0.58, 95% CI 0.36-0.93; p = 0.02; I 2 = 73%).
Conclusion: In patients with nosocomial infections, PMB is not superior to other antibiotics in terms of mortality, specifically when compared to ceftazidime-avibactam. However, PMB demonstrated an advantage in terms of nephrotoxicity compared to colistin.
Keywords: Polymyxin B; ceftazidime-avibactam; colistin; meta-analysis; nosocomial infections; tigecycline.
Copyright © 2024 Peng, Zhang, Qi, Zhong, Sun, Chen, Zhu, Lv and Ma.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Evaluation of the in vitro synergy of polymyxin B-based combinations against polymyxin B -resistant gram-negative bacilli.Microb Pathog. 2022 May;166:105517. doi: 10.1016/j.micpath.2022.105517. Epub 2022 Apr 7. Microb Pathog. 2022. PMID: 35398467
-
Efficacy and Safety of Ceftazidime-Avibactam for the Treatment of Carbapenem-Resistant Enterobacterales Bloodstream Infection: a Systematic Review and Meta-Analysis.Microbiol Spectr. 2022 Apr 27;10(2):e0260321. doi: 10.1128/spectrum.02603-21. Epub 2022 Apr 4. Microbiol Spectr. 2022. PMID: 35377233 Free PMC article.
-
Ceftazidime/Avibactam-Based Versus Polymyxin B-Based Therapeutic Regimens for the Treatment of Carbapenem-Resistant Klebsiella pneumoniae Infection in Critically Ill Patients: A Retrospective Cohort Study.Infect Dis Ther. 2022 Oct;11(5):1917-1934. doi: 10.1007/s40121-022-00682-0. Epub 2022 Aug 17. Infect Dis Ther. 2022. PMID: 35976531 Free PMC article.
-
Clinical outcomes and safety of intravenous polymyxin B-based treatment in critically ill patients with carbapenem-resistant Acinetobacter baumannii nosocomial pneumonia.Int J Antimicrob Agents. 2023 Aug;62(2):106880. doi: 10.1016/j.ijantimicag.2023.106880. Epub 2023 Jun 9. Int J Antimicrob Agents. 2023. PMID: 37301311
-
Efficacy and safety of ceftazidime-avibactam versus polymyxins in the treatment of carbapenem-resistant Enterobacteriaceae infection: a systematic review and meta-analysis.BMJ Open. 2023 May 3;13(5):e070491. doi: 10.1136/bmjopen-2022-070491. BMJ Open. 2023. PMID: 37137556 Free PMC article.
Cited by
-
Improving health literacy and stakeholder-directed knowledge of One Health through analysis of readability: a cross sectional infodemiology study.Sci One Health. 2024 Nov 7;3:100088. doi: 10.1016/j.soh.2024.100088. eCollection 2024. Sci One Health. 2024. PMID: 39633846 Free PMC article.
-
Biomarker-Driven Pharmacokinetics and Efficacy of Polymyxin B in Critically Ill Patients with XDR-GN Pneumonia.Pharmaceuticals (Basel). 2025 Apr 17;18(4):586. doi: 10.3390/ph18040586. Pharmaceuticals (Basel). 2025. PMID: 40284021 Free PMC article.
References
LinkOut - more resources
Full Text Sources