

Non-invasive assessment of left ventricular contractility by myocardial work index in veno-arterial membrane oxygenation patients: rationale and design of the MIX-ECMO multicentre observational study
- PMID: 38863897
- PMCID: PMC11165188
- DOI: 10.3389/fcvm.2024.1399874
Non-invasive assessment of left ventricular contractility by myocardial work index in veno-arterial membrane oxygenation patients: rationale and design of the MIX-ECMO multicentre observational study
Abstract
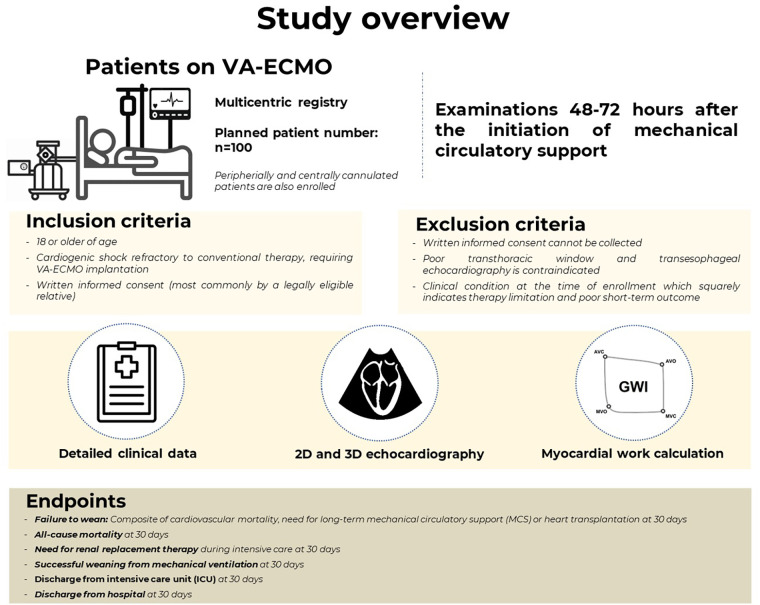
Introduction and aims: Veno-arterial extracorporeal membrane oxygenation (VA-ECMO) is an increasingly utilized therapeutic choice in patients with cardiogenic shock, however, high complication rate often counteracts with its beneficial cardiopulmonary effects. The assessment of left ventricular (LV) function in key in the management of this population, however, the most commonly used measures of LV performance are substantially load-dependent. Non-invasive myocardial work is a novel LV functional measure which may overcome this limitation and estimate LV function independent of the significantly altered loading conditions of VA-ECMO therapy. The Usefulness of Myocardial Work IndeX in ExtraCorporeal Membrane Oxygenation Patients (MIX-ECMO) study aims to examine the prognostic role of non-invasive myocardial work in VA-ECMO-supported patients.
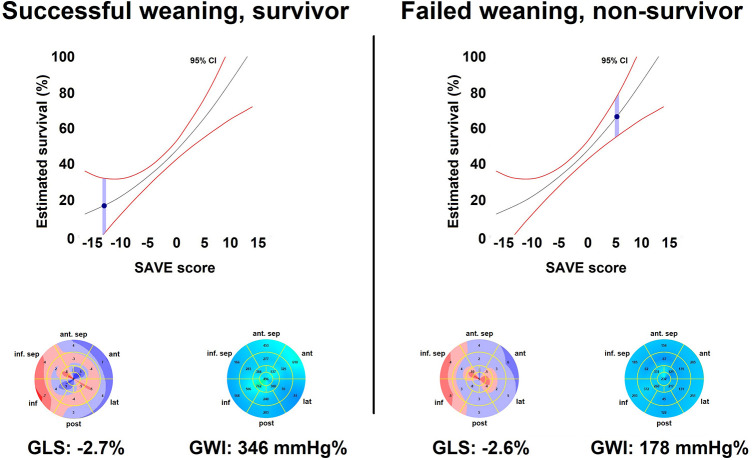
Methods: The MIX-ECMO is a multicentric, prospective, observational study. We aim to enroll 110 patients 48-72 h after the initiation of VA-ECMO support. The patients will undergo a detailed echocardiographic examination and a central echocardiography core laboratory will quantify conventional LV functional measures and non-invasive myocardial work parameters. The primary endpoint will be failure to wean at 30 days as a composite of cardiovascular mortality, need for long-term mechanical circulatory support or heart transplantation at 30 days, and besides that other secondary objectives will also be investigated. Detailed clinical data will also be collected to compare LV functional measures to parameters with established prognostic role and also to the Survival After Veno-arterial-ECMO (SAVE) score.
Conclusions: The MIX-ECMO study will be the first to determine if non-invasive myocardial work has added prognostic value in patients receiving VA-ECMO support.
Keywords: critical care; echocardiography; extracorporeal membrane oxygenation; myocardial work index; speckle-tracking echocardiography.
© 2024 Lakatos, Ladányi, Fábián, Ehrenberger, Turschl, Bagyura, Evrard, Vandroux, Goudelin, Lindner, Britsch, Dürschmied, Zima, Csikós, Túróczi, Soltész, Németh, Kovács, Édes and Merkely.
Conflict of interest statement
BKL, AF and AK report personal fees from Argus Cognitive Inc., outside the submitted report. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Yannopoulos D, Bartos J, Raveendran G, Walser E, Connett J, Murray TA, et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): a phase 2, single centre, open-label, randomised controlled trial. Lancet. (2020) 396:1807–16. 10.1016/S0140-6736(20)32338-2 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources