

Pathological characteristics of reoperated regrowing clinically nonfunctioning pituitary tumor cases in comparison with initial surgical cases
- PMID: 38863935
- PMCID: PMC11165050
- DOI: 10.3389/fendo.2024.1400671
Pathological characteristics of reoperated regrowing clinically nonfunctioning pituitary tumor cases in comparison with initial surgical cases
Abstract
Objective: Postoperative nonfunctioning pituitary tumor (NFPT) regrowth is a significant concern, but its predictive factors are not well established. This study aimed to elucidate the pathological characteristics of NFPTs indicated for reoperation for tumor regrowth.
Methods: Pathological, radiological, and clinical data were collected from patients who underwent repeat operation for NFPT at Moriyama Memorial Hospital (MMH) between April 2018 and September 2023. For comparison, we also gathered data from patients who underwent initial surgery for NFPT during the same period at MMH.
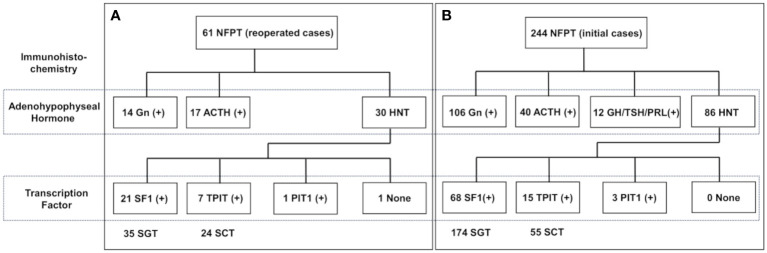
Results: Overall, 61 and 244 NFPT patients who respectively underwent reoperation and initial operation were evaluated. The mean period between the previous operation and reoperation was 113 months. Immunonegativity for any adenohypophyseal hormone was significantly more frequent in the reoperation group than in the initial operation group. In addition, the rate of hormone-negative but transcription factor-positive (H-/TF+) tumors among silent gonadotroph tumors was significantly higher in the reoperation group than in the initial operation group. Furthermore, seven silent corticotroph tumors (SCTs) in the reoperation group were ACTH-negative but TPIT-positive. Because most of the previous surgeries were performed in other hospitals a long time ago, we could procure the previous pathological results with immunohistochemistry (IHC) only from 21 patients. IHC for TF had not been performed in all the previous specimens. IHC for adenohypophyseal hormone was almost the same as the current results, and many H-/TF+ tumors were previously diagnosed as NCT. In addition, the reoperated patients were classified into 3 groups on the basis of the condition of the previous operation: gross total resection (GTR), 12 patients; subtotal resection (STR), 17 patients; and partial resection (PR), 32 patients. The mean Ki-67 LI in the GTR, STR, and PR subgroups were 1.82, 1.37, and 0.84, respectively, with the value being significantly higher in the GTR subgroup than in the PR subgroup (P < 0.05).
Conclusions: The ratio of H-/TF+ tumors is significantly higher in symptomatically regrown tumors than in the initial cases, which used to be diagnosed as NCT. PR cases tend to grow symptomatically in a shorter period, even with lower Ki-67 LI than GTR cases.
Keywords: gross total resection; nonfunctioning pituitary tumor; null cell tumor; regrowth; silent corticotroph tumor; silent gonadotroph tumors; transcription factor.
Copyright © 2024 Ishida, Inoshita, Tanabe, Takano, Tanaka-Mizuno, Kato, Yoshimoto, Shiramizu, Matsuoka and Yamada.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Intraoperative high-field MRI for transsphenoidal reoperations of nonfunctioning pituitary adenoma.J Neurosurg. 2014 Nov;121(5):1166-75. doi: 10.3171/2014.6.JNS131994. Epub 2014 Aug 15. J Neurosurg. 2014. PMID: 25127413
-
Endoscopic endonasal approach for craniopharyngioma: the importance of the relationship between pituitary stalk and tumor.J Neurosurg. 2018 Sep;129(3):611-619. doi: 10.3171/2017.4.JNS162143. Epub 2017 Sep 29. J Neurosurg. 2018. PMID: 28960155
-
Endonasal endoscopic reoperation for residual or recurrent craniopharyngiomas.J Neurosurg. 2017 Feb;126(2):418-430. doi: 10.3171/2016.1.JNS152238. Epub 2016 May 6. J Neurosurg. 2017. PMID: 27153172
-
Endoscopic Endonasal Approach to Giant Pituitary Adenomas: Surgical Outcomes and Review of the Literature.World Neurosurg. 2021 May;149:e1043-e1055. doi: 10.1016/j.wneu.2021.01.019. Epub 2021 Jan 29. World Neurosurg. 2021. PMID: 33524611 Review.
-
The behavior of residual tumors and facial nerve outcomes after incomplete excision of vestibular schwannomas.J Neurosurg. 2014 Jun;120(6):1278-87. doi: 10.3171/2014.2.JNS131497. Epub 2014 Apr 11. J Neurosurg. 2014. PMID: 24724851 Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous