

No improvement in mortality among critically ill patients with carbapenems as initial empirical therapy and more detection of multi-drug resistant pathogens associated with longer use: a post hoc analysis of a prospective cohort study
- PMID: 38864641
- PMCID: PMC11218456
- DOI: 10.1128/spectrum.00342-24
No improvement in mortality among critically ill patients with carbapenems as initial empirical therapy and more detection of multi-drug resistant pathogens associated with longer use: a post hoc analysis of a prospective cohort study
Abstract
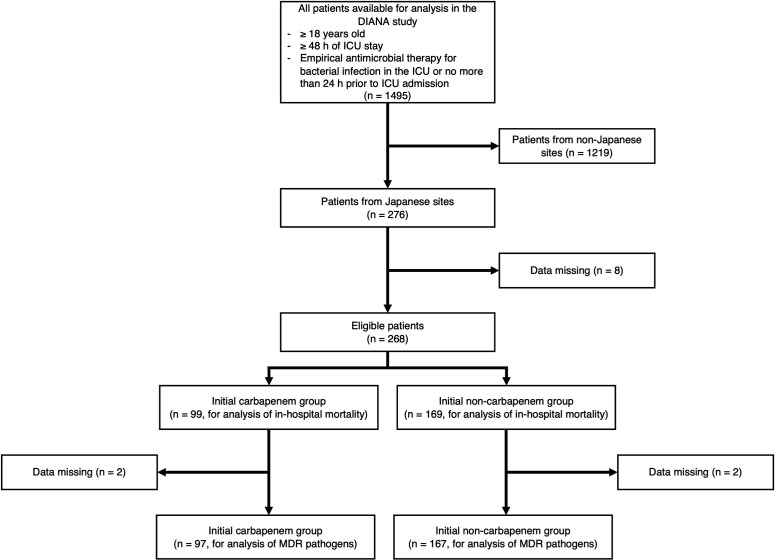
Whether empirical therapy with carbapenems positively affects the outcomes of critically ill patients with bacterial infections remains unclear. This study aimed to investigate whether the use of carbapenems as the initial antimicrobial administration reduces mortality and whether the duration of carbapenem use affects the detection of multidrug-resistant (MDR) pathogens. This was a post hoc analysis of data acquired from Japanese participating sites from a multicenter, prospective observational study [Determinants of Antimicrobial Use and De-escalation in Critical Care (DIANA study)]. A total of 268 adult patients with clinically suspected or confirmed bacterial infections from 31 Japanese intensive care units (ICUs) were analyzed. The patients were divided into two groups: patients who were administered carbapenems as initial antimicrobials (initial carbapenem group, n = 99) and those who were not administered carbapenems (initial non-carbapenem group, n = 169). The primary outcomes were mortality at day 28 and detection of MDR pathogens. Multivariate logistic regression analysis revealed that mortality at day 28 did not differ between the two groups [18 (18%) vs 27 (16%), respectively; odds ratio: 1.25 (95% confidence interval (CI): 0.59-2.65), P = 0.564]. The subdistribution hazard ratio for detecting MDR pathogens on day 28 per additional day of carbapenem use is 1.08 (95% CI: 1.05-1.13, P < 0.001 using the Fine-Gray model with death regarded as a competing event). In conclusion, in-hospital mortality was similar between the groups, and a longer duration of carbapenem use as the initial antimicrobial therapy resulted in a higher risk of detection of new MDR pathogens.IMPORTANCEWe found no statistical difference in mortality with the empirical use of carbapenems as initial antimicrobial therapy among critically ill patients with bacterial infections. Our study revealed a lower proportion of inappropriate initial antimicrobial administrations than those reported in previous studies. This result suggests the importance of appropriate risk assessment for the involvement of multidrug-resistant (MDR) pathogens and the selection of suitable antibiotics based on risk. To the best of our knowledge, this study is the first to demonstrate that a longer duration of carbapenem use as initial therapy is associated with a higher risk of subsequent detection of MDR pathogens. This finding underscores the importance of efforts to minimize the duration of carbapenem use as initial antimicrobial therapy when it is necessary.
Keywords: carbapenem; critically ill; infectious disease; initial empirical therapy; intensive care unit; multidrug resistance.
Conflict of interest statement
The authors declare no conflict of interest.
Similar articles
-
Carbapenems and subsequent multiresistant bloodstream infection: does treatment duration matter?Int J Antimicrob Agents. 2009 Sep;34(3):246-51. doi: 10.1016/j.ijantimicag.2009.04.007. Int J Antimicrob Agents. 2009. PMID: 19628129
-
Use of broad-spectrum antimicrobials for more than 72 h and the detection of multidrug-resistant bacteria in Japanese intensive care units: a multicenter retrospective cohort study.Antimicrob Resist Infect Control. 2022 Sep 29;11(1):119. doi: 10.1186/s13756-022-01146-3. Antimicrob Resist Infect Control. 2022. PMID: 36175948 Free PMC article.
-
Empirical carbapenems or piperacillin/tazobactam for infections in intensive care: An international retrospective cohort study.Acta Anaesthesiol Scand. 2024 Jul;68(6):821-829. doi: 10.1111/aas.14419. Epub 2024 Mar 28. Acta Anaesthesiol Scand. 2024. PMID: 38549422
-
Carbapenem use in critically ill patients.Curr Opin Infect Dis. 2020 Feb;33(1):86-91. doi: 10.1097/QCO.0000000000000622. Curr Opin Infect Dis. 2020. PMID: 31815750 Review.
-
Risk factors for hospitalized patients with resistant or multidrug-resistant Pseudomonas aeruginosa infections: a systematic review and meta-analysis.Antimicrob Resist Infect Control. 2018 Jul 4;7:79. doi: 10.1186/s13756-018-0370-9. eCollection 2018. Antimicrob Resist Infect Control. 2018. PMID: 29997889 Free PMC article.
References
-
- Ferrer R, Martin-Loeches I, Phillips G, Osborn TM, Townsend S, Dellinger RP, Artigas A, Schorr C, Levy MM. 2014. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit Care Med 42:1749–1755. doi:10.1097/CCM.0000000000000330 - DOI - PubMed
-
- Kumar A, Ellis P, Arabi Y, Roberts D, Light B, Parrillo JE, Dodek P, Wood G, Kumar A, Simon D, Peters C, Ahsan M, Chateau D, Cooperative Antimicrobial Therapy of Septic Shock Database Research Group . 2009. Initiation of inappropriate antimicrobial therapy results in a fivefold reduction of survival in human septic shock. Chest 136:1237–1248. doi:10.1378/chest.09-0087 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
