

Open Retromuscular Sugarbaker vs Keyhole Mesh Placement for Parastomal Hernia Repair: A Randomized Clinical Trial
- PMID: 38865142
- PMCID: PMC11170450
- DOI: 10.1001/jamasurg.2024.1686
Open Retromuscular Sugarbaker vs Keyhole Mesh Placement for Parastomal Hernia Repair: A Randomized Clinical Trial
Abstract
Importance: Durable parastomal hernia repair remains elusive. There is limited evidence comparing the durability of the open retromuscular Sugarbaker and keyhole mesh configurations.
Objective: To determine if the open retromuscular Sugarbaker mesh placement technique would lower parastomal hernia recurrence rates.
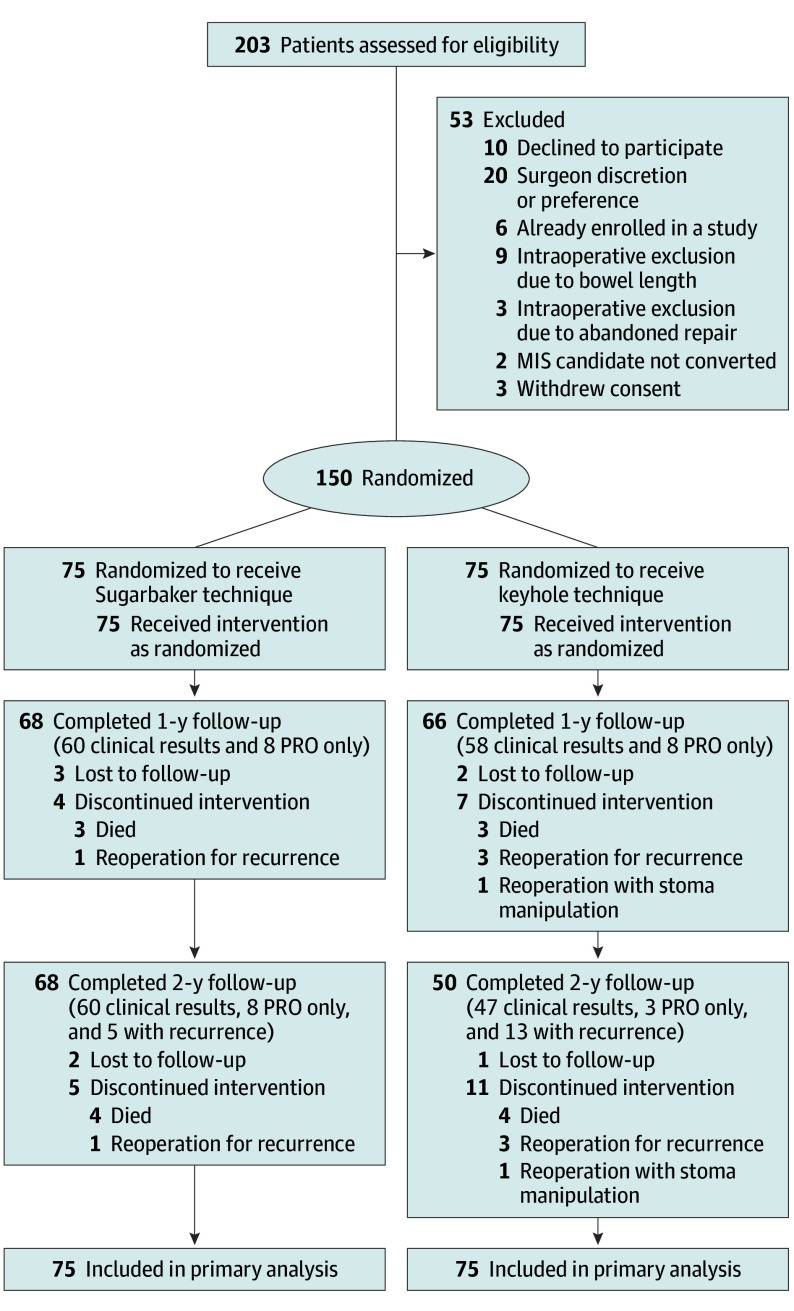
Design, setting, and participants: In this single-center, randomized clinical trial, 150 patients with a permanent stoma and associated parastomal hernia who were candidates for open retromuscular parastomal hernia repair were enrolled and randomized from April 2019 to April 2022 and followed up for 2 years.
Interventions: Following intraoperative assessment to determine the feasibility of either technique, enrolled patients were randomized to receive either retromuscular Sugarbaker or keyhole synthetic mesh placement.
Main outcomes and measures: The primary outcome was parastomal hernia recurrence at 2 years. Secondary outcomes included mesh-related complications, wound complications, reoperations, as well as patient-reported pain, abdominal wall-specific quality of life, stoma-specific quality of life, and decision regret at 1 year and 2 years.
Results: A total of 150 patients were randomized, and with 91% follow-up at 2 years, there were 13 (17%) parastomal hernia recurrences in the retromuscular Sugarbaker arm and 18 (24%) in the keyhole arm (adjusted risk difference, -0.029; 95% CI, -0.17 to 0.153, and adjusted risk ratio, 0.87; 95% CI, 0.42 to 1.69). There were no statistically significant differences between the Sugarbaker and keyhole groups regarding reoperations for recurrence (2 vs 7, respectively), nonhernia intra-abdominal pathology (4 vs 10, respectively), stoma necrosis (1 vs 0, respectively), mesh-related complications (4 vs 1, respectively), patient-reported pain, abdominal wall-specific quality of life, stoma-specific quality of life, and decision regret at any time point.
Conclusions and relevance: In the setting of open parastomal hernia repair, a retromuscular Sugarbaker mesh placement technique was not superior to a keyhole configuration 2 years after repair. Further innovation is necessary to improve parastomal hernia repair outcomes.
Trial registration: ClinicalTrials.gov Identifier: NCT03972553.
Conflict of interest statement
Figures

Comment on
-
Parastomal Hernias-A Recurring Problem for Surgeons and Patients.JAMA Surg. 2024 Sep 1;159(9):989. doi: 10.1001/jamasurg.2024.1683. JAMA Surg. 2024. PMID: 38865145 No abstract available.
References
-
- United Ostomy Associations of America . What is an ostomy? Accessed January 7, 2024. https://www.ostomy.org/what-is-an-ostomy
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
