

Heterotypic immunity from prior SARS-CoV-2 infection but not COVID-19 vaccination associates with lower endemic coronavirus incidence
- PMID: 38865483
- PMCID: PMC11565543
- DOI: 10.1126/scitranslmed.ado7588
Heterotypic immunity from prior SARS-CoV-2 infection but not COVID-19 vaccination associates with lower endemic coronavirus incidence
Abstract
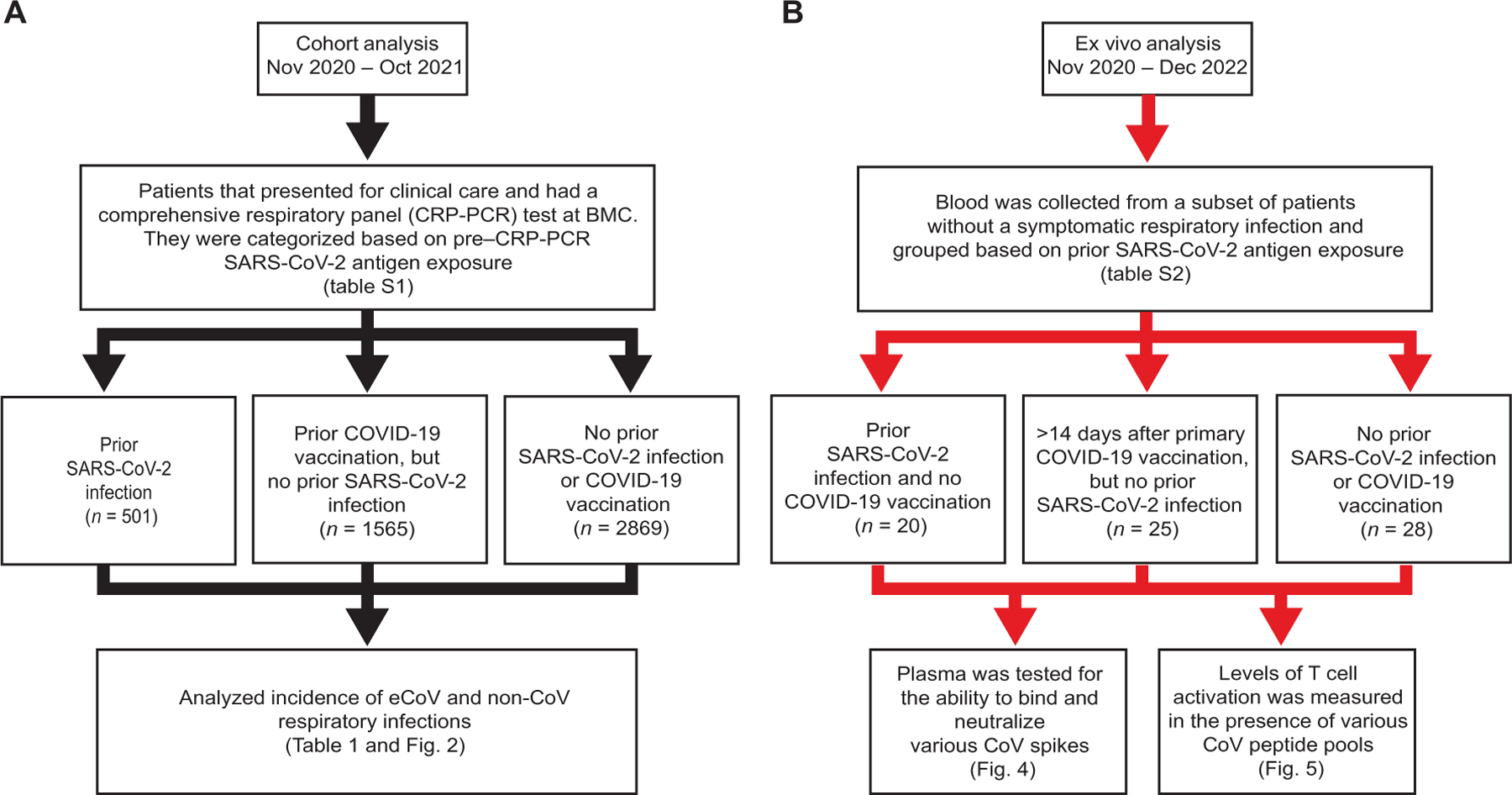
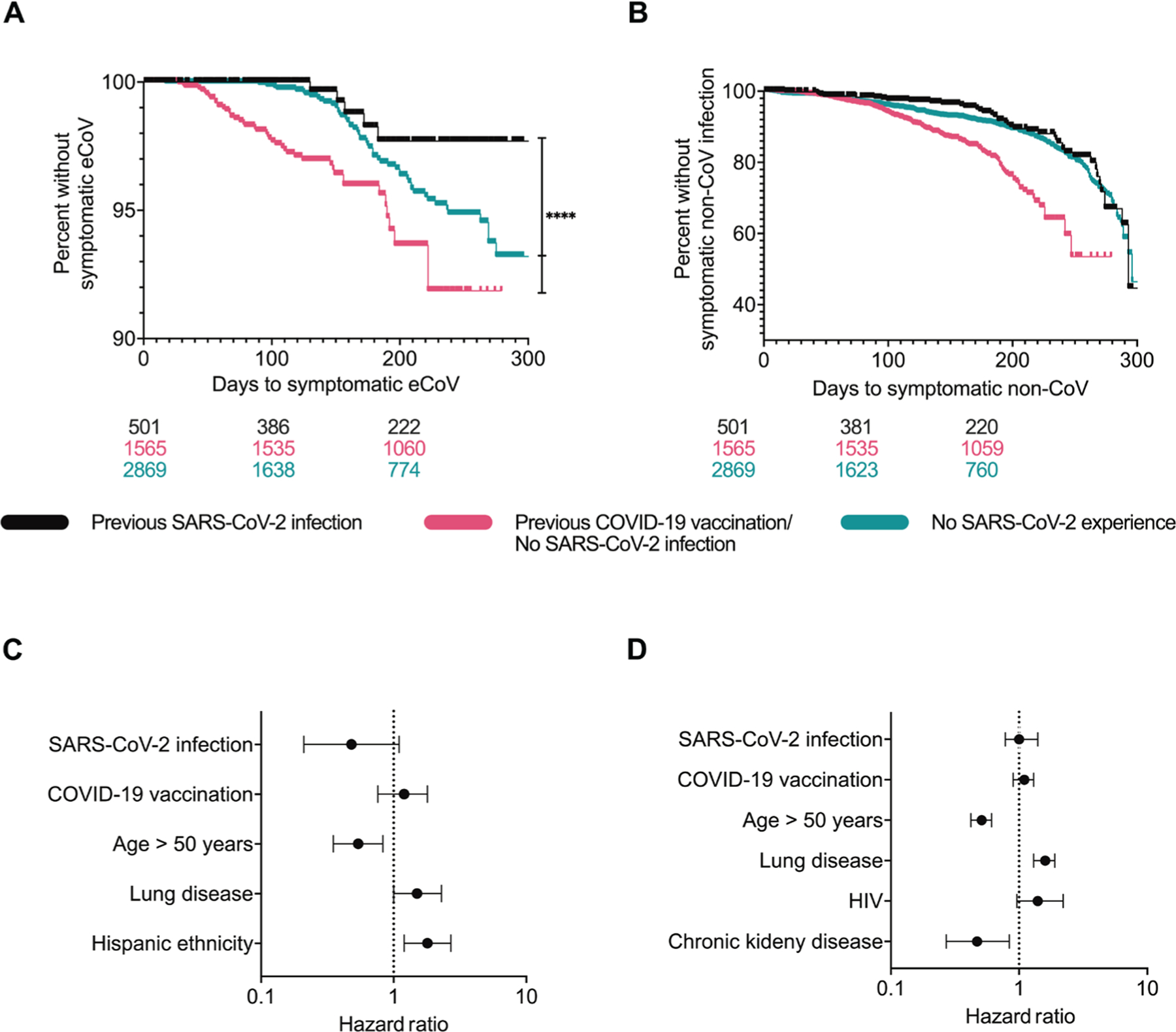
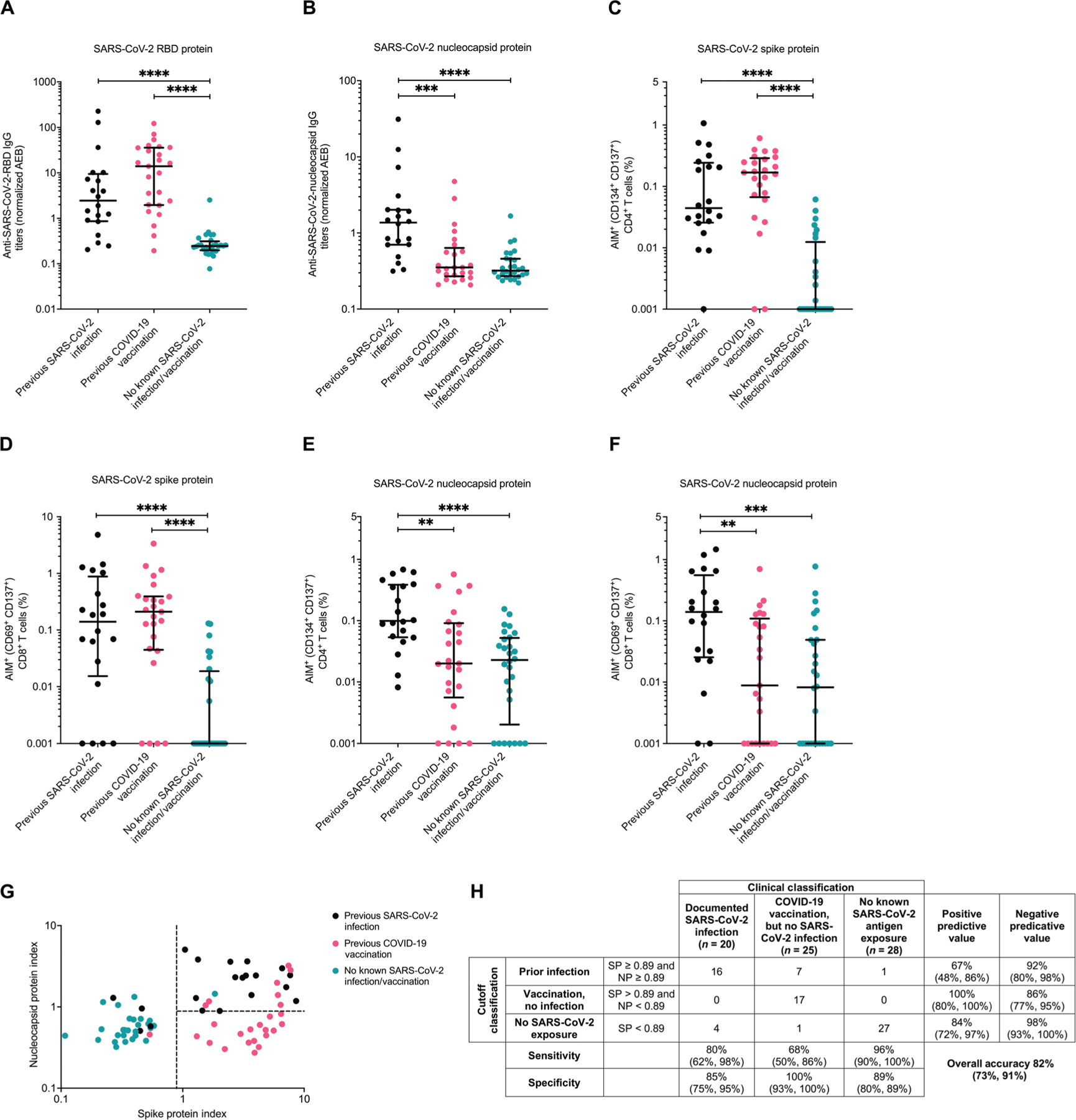
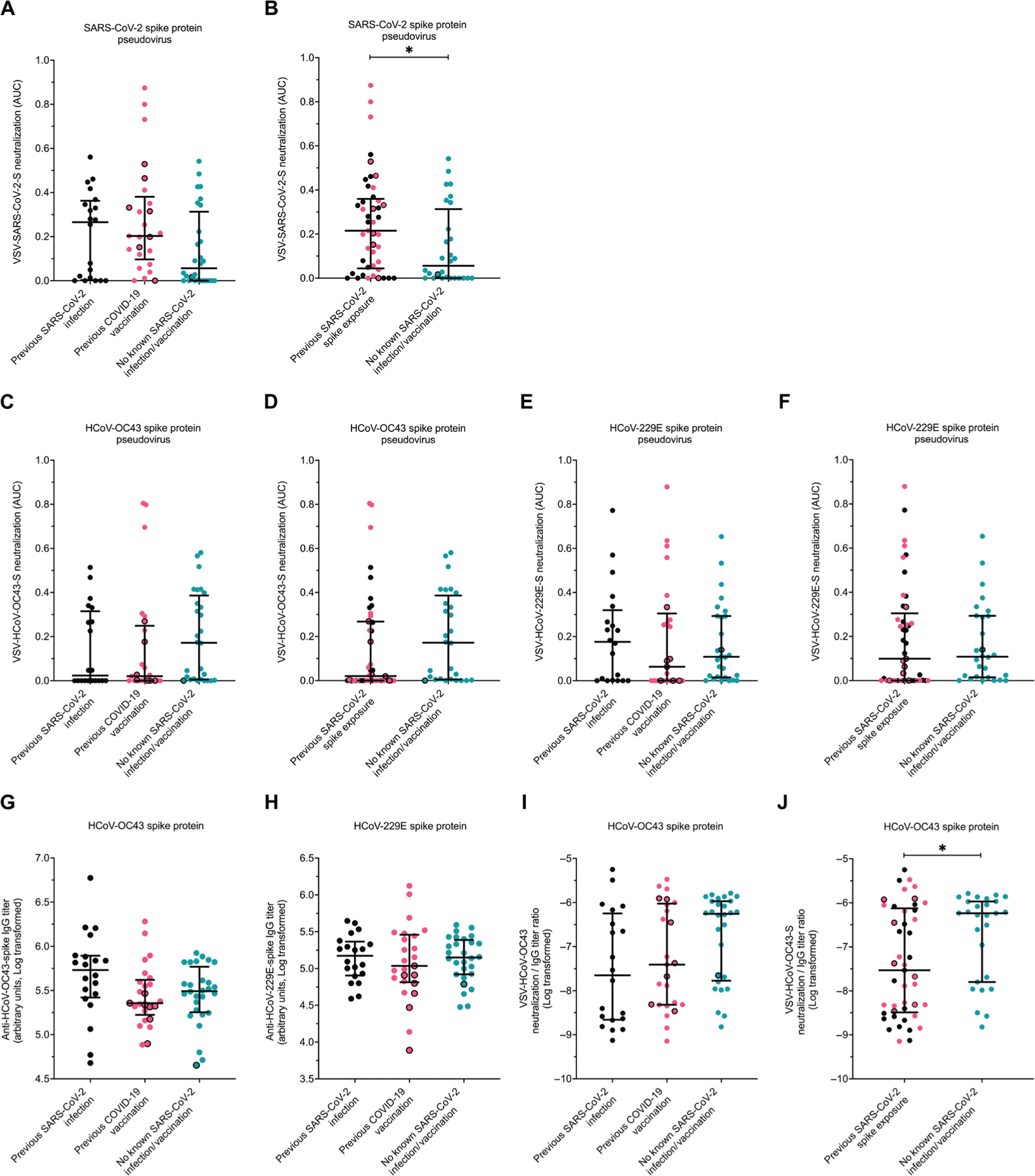
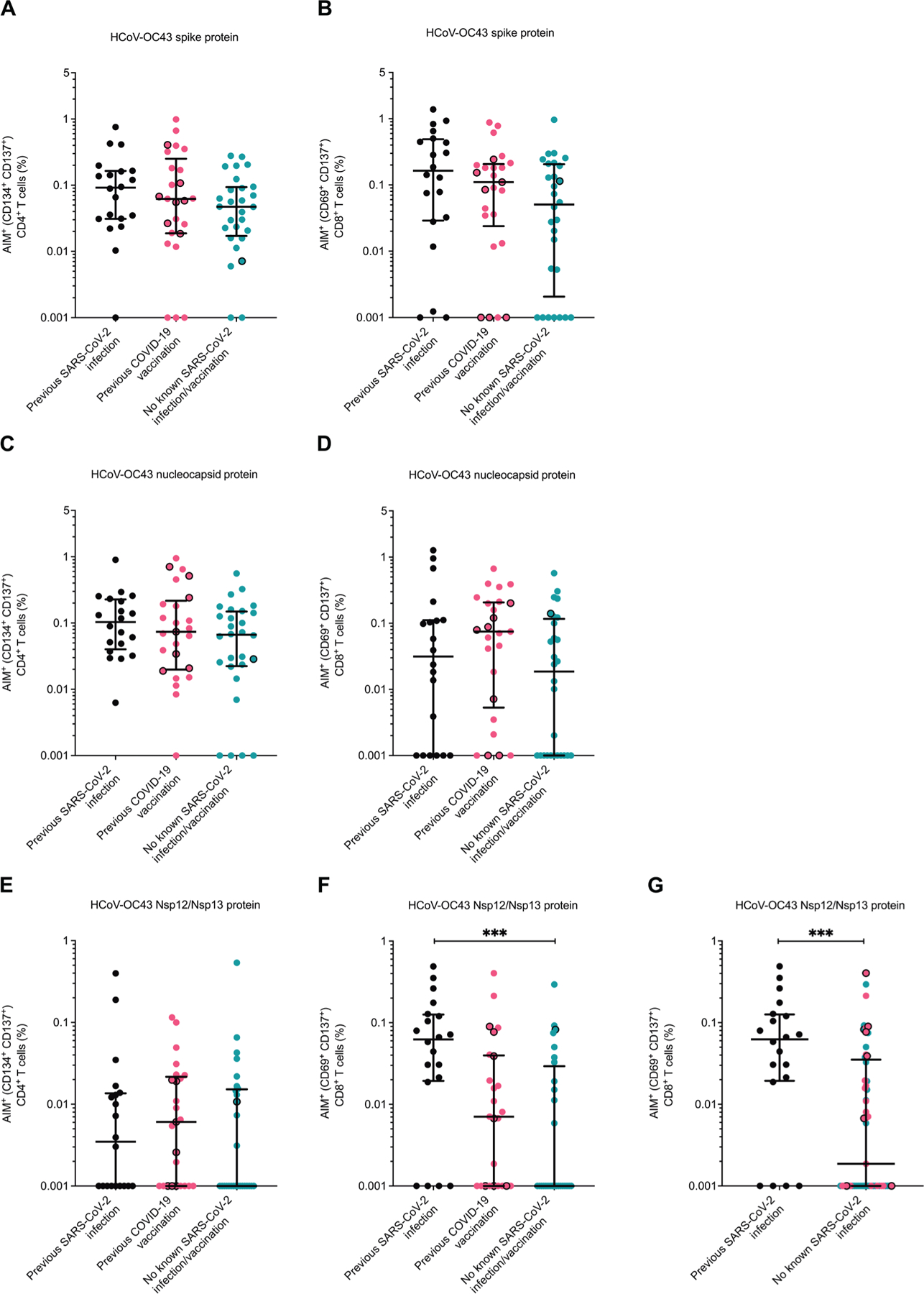
Immune responses from prior severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and COVID-19 vaccination mitigate disease severity, but they do not fully prevent subsequent infections, especially from genetically divergent strains. We examined the incidence of and immune differences against human endemic coronaviruses (eCoVs) as a proxy for response against future genetically heterologous coronaviruses (CoVs). We assessed differences in symptomatic eCoV and non-CoV respiratory disease incidence among those with known prior SARS-CoV-2 infection or previous COVID-19 vaccination but no documented SARS-CoV-2 infection or neither exposure. Retrospective cohort analyses suggest that prior SARS-CoV-2 infection, but not previous COVID-19 vaccination alone, associates with a lower incidence of subsequent symptomatic eCoV infection. There was no difference in non-CoV incidence, implying that the observed difference was eCoV specific. In a second cohort where both cellular and humoral immunity were measured, those with prior SARS-CoV-2 spike protein exposure had lower eCoV-directed neutralizing antibodies, suggesting that neutralization is not responsible for the observed decreased eCoV disease. The three groups had similar cellular responses against the eCoV spike protein and nucleocapsid antigens. However, CD8+ T cell responses to the nonstructural eCoV proteins nsp12 and nsp13 were higher in individuals with previous SARS-CoV-2 infection as compared with the other groups. This association between prior SARS-CoV-2 infection and decreased incidence of eCoV disease may therefore be due to a boost in CD8+ T cell responses against eCoV nsp12 and nsp13, suggesting that incorporation of nonstructural viral antigens in a future pan-CoV vaccine may improve vaccine efficacy.
Conflict of interest statement
Figures
Update of
-
Heterotypic responses against nsp12/nsp13 from prior SARS-CoV-2 infection associates with lower subsequent endemic coronavirus incidence.bioRxiv [Preprint]. 2023 Oct 24:2023.10.23.563621. doi: 10.1101/2023.10.23.563621. bioRxiv. 2023. Update in: Sci Transl Med. 2024 Jun 12;16(751):eado7588. doi: 10.1126/scitranslmed.ado7588. PMID: 37961343 Free PMC article. Updated. Preprint.
Similar articles
-
Endemic coronavirus infection is associated with SARS-CoV-2 Fc receptor-binding antibodies.J Virol. 2025 Jun 17;99(6):e0055025. doi: 10.1128/jvi.00550-25. Epub 2025 May 19. J Virol. 2025. PMID: 40387363 Free PMC article.
-
Heterotypic responses against nsp12/nsp13 from prior SARS-CoV-2 infection associates with lower subsequent endemic coronavirus incidence.bioRxiv [Preprint]. 2023 Oct 24:2023.10.23.563621. doi: 10.1101/2023.10.23.563621. bioRxiv. 2023. Update in: Sci Transl Med. 2024 Jun 12;16(751):eado7588. doi: 10.1126/scitranslmed.ado7588. PMID: 37961343 Free PMC article. Updated. Preprint.
-
Anti-SARS-CoV-2 total immunoglobulin and neutralising antibody responses in healthy blood donors throughout the COVID-19 pandemic: a longitudinal observational study.Swiss Med Wkly. 2024 Jul 1;154:3408. doi: 10.57187/s.3408. Swiss Med Wkly. 2024. PMID: 39137369
-
Antibody tests for identification of current and past infection with SARS-CoV-2.Cochrane Database Syst Rev. 2022 Nov 17;11(11):CD013652. doi: 10.1002/14651858.CD013652.pub2. Cochrane Database Syst Rev. 2022. PMID: 36394900 Free PMC article.
-
SARS-CoV-2-neutralising monoclonal antibodies to prevent COVID-19.Cochrane Database Syst Rev. 2022 Jun 17;6(6):CD014945. doi: 10.1002/14651858.CD014945.pub2. Cochrane Database Syst Rev. 2022. PMID: 35713300 Free PMC article.
Cited by
-
Comprehensive analysis of human coronavirus antibody responses in ICU and non-ICU COVID-19 patients reveals IgG3 against SARS-CoV-2 spike protein as a key biomarker of disease severity.J Med Microbiol. 2025 May;74(5):002012. doi: 10.1099/jmm.0.002012. J Med Microbiol. 2025. PMID: 40359129 Free PMC article.
-
The effect of SARS-CoV-2 and influenza vaccination on endemic coronavirus-related mortality: A retrospective cohort study in Brazil.Hum Vaccin Immunother. 2025 Dec;21(1):2516314. doi: 10.1080/21645515.2025.2516314. Epub 2025 Jun 11. Hum Vaccin Immunother. 2025. PMID: 40497727 Free PMC article.
-
Endemic coronavirus infection is associated with SARS-CoV-2 Fc receptor-binding antibodies.J Virol. 2025 Jun 17;99(6):e0055025. doi: 10.1128/jvi.00550-25. Epub 2025 May 19. J Virol. 2025. PMID: 40387363 Free PMC article.
-
Improving health literacy and stakeholder-directed knowledge of One Health through analysis of readability: a cross sectional infodemiology study.Sci One Health. 2024 Nov 7;3:100088. doi: 10.1016/j.soh.2024.100088. eCollection 2024. Sci One Health. 2024. PMID: 39633846 Free PMC article.
-
Common Cold Coronavirus Test Positivity Decreased After Widespread SARS-CoV-2 Experience.Open Forum Infect Dis. 2025 Jun 18;12(7):ofaf326. doi: 10.1093/ofid/ofaf326. eCollection 2025 Jul. Open Forum Infect Dis. 2025. PMID: 40599488 Free PMC article.
References
-
- Fung TS, Liu DX, Similarities and dissimilarities of COVID-19 and other coronavirus diseases. Annu. Rev. Microbiol 75, 19–47 (2021). - PubMed
-
- Andrews N, Tessier E, Stowe J, Gower C, Kirsebom F, Simmons R, Gallagher E, Thelwall S, Groves N, Dabrera G, Myers R, Campbell CNJ, Amirthalingam G, Edmunds M, Zambon M, Brown K, Hopkins S, Chand M, Ladhani SN, Ramsay M, Lopez Bernal J, Duration of protection against mild and severe disease by Covid-19 vaccines. N. Engl. J. Med 386, 340–350 (2022). - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
