

Profiling Bacteria in the Lungs of Patients with Severe Influenza Versus COVID-19 with or without Aspergillosis
- PMID: 38865563
- PMCID: PMC11568435
- DOI: 10.1164/rccm.202401-0145OC
Profiling Bacteria in the Lungs of Patients with Severe Influenza Versus COVID-19 with or without Aspergillosis
Abstract
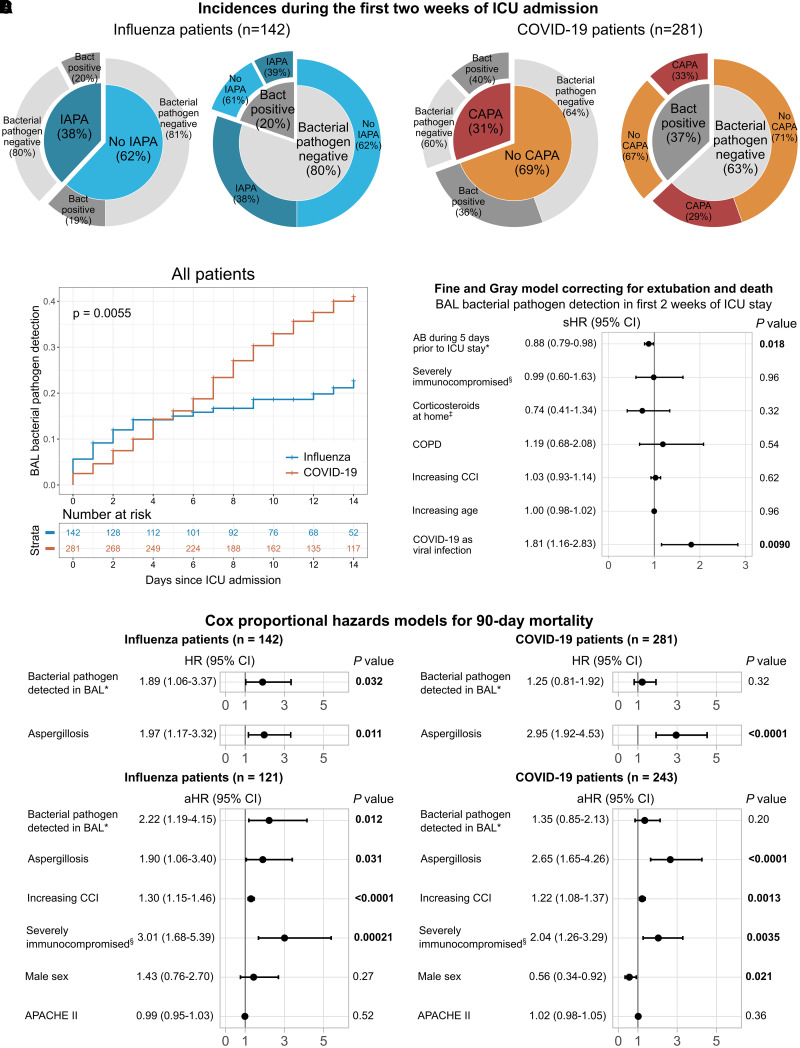
Rationale: The influence of the lung bacterial microbiome, including potential pathogens, in patients with influenza-associated pulmonary aspergillosis (IAPA) or coronavirus disease (COVID-19)-associated pulmonary aspergillosis (CAPA) has yet to be explored. Objectives: To explore the composition of the lung bacterial microbiome and its association with viral and fungal infection, immunity, and outcome in severe influenza versus COVID-19 with or without aspergillosis. Methods: We performed a retrospective study in mechanically ventilated patients with influenza and COVID-19 with or without invasive aspergillosis in whom BAL for bacterial culture (with or without PCR) was obtained within 2 weeks after ICU admission. In addition, 16S rRNA gene sequencing data and viral and bacterial load of BAL samples from a subset of these patients, and of patients requiring noninvasive ventilation, were analyzed. We integrated 16S rRNA gene sequencing data with existing immune parameter datasets. Measurements and Main Results: Potential bacterial pathogens were detected in 20% (28/142) of patients with influenza and 37% (104/281) of patients with COVID-19, whereas aspergillosis was detected in 38% (54/142) of patients with influenza and 31% (86/281) of patients with COVID-19. A significant association between bacterial pathogens in BAL fluid and 90-day mortality was found only in patients with influenza, particularly patients with IAPA. Patients with COVID-19, but not patients with influenza, showed increased proinflammatory pulmonary cytokine responses to bacterial pathogens. Conclusions: Aspergillosis is more frequently detected in the lungs of patients with severe influenza than bacterial pathogens. Detection of bacterial pathogens associates with worse outcome in patients with influenza, particularly in those with IAPA, but not in patients with COVID-19. The immunological dynamics of tripartite viral-fungal-bacterial interactions deserve further investigation.
Keywords: COVID-19; aspergillosis; immunology; influenza; microbiome.
Figures



Comment in
-
One for All and All for One: Multikingdom Interplay in Severe Viral Pneumonia.Am J Respir Crit Care Med. 2024 Nov 15;210(10):1176-1178. doi: 10.1164/rccm.202406-1237ED. Am J Respir Crit Care Med. 2024. PMID: 39078170 Free PMC article. No abstract available.
References
-
- Paget J, Spreeuwenberg P, Charu V, Taylor RJ, Iuliano AD, Bresee J, et al. Global Seasonal Influenza-associated Mortality Collaborator Network and GLaMOR Collaborating Teams Global mortality associated with seasonal influenza epidemics: new burden estimates and predictors from the GLaMOR Project. J Glob Health . 2019;9:020421. - PMC - PubMed
-
- Schauwvlieghe AFAD, Rijnders BJA, Philips N, Verwijs R, Vanderbeke L, Van Tienen C, et al. Dutch-Belgian Mycosis study group Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: a retrospective cohort study. Lancet Respir Med . 2018;6:782–792. - PubMed
MeSH terms
Substances
Grants and funding
- G053121N/Fonds Wetenschappelijk Onderzoek/United States
- "Coronafonds"/Universitaire Ziekenhuizen Leuven, KU Leuven/United States
- 2022.06674.PTDC/Fundação para a Ciência e a Tecnologia/United States
- CEECIND/04058/2018/Fundação para a Ciência e a Tecnologia/United States
- "la Caixa" Foundation/United States
- 847507/Horizon 2020 Framework Programme/United States
- CPP2021-008552/Ministerio de Ciencia e Innovación/United States
- SGR01551/Agència de Gestió d'Ajuts Universitaris i de Recerca/United States
- GBMF9742/Gordon and Betty Moore Foundation/United States
- LCF/PR/HR21/00737/"La Caixa" foundation/United States
- CIBERINFEC CB21/13/00061-ISCIII-SGEFI/ERDF/Instituto de Salud Carlos III/United States
LinkOut - more resources
Full Text Sources
Medical
