

Tumour microenvironment characterisation to stratify patients for hyperthermic intraperitoneal chemotherapy in high-grade serous ovarian cancer (OVHIPEC-1)
- PMID: 38866963
- PMCID: PMC11300911
- DOI: 10.1038/s41416-024-02731-6
Tumour microenvironment characterisation to stratify patients for hyperthermic intraperitoneal chemotherapy in high-grade serous ovarian cancer (OVHIPEC-1)
Abstract
Background: Hyperthermic intraperitoneal chemotherapy (HIPEC) improves survival in patients with Stage III ovarian cancer following interval cytoreductive surgery (CRS). Optimising patient selection is essential to maximise treatment efficacy and avoid overtreatment. This study aimed to identify biomarkers that predict HIPEC benefit by analysing gene signatures and cellular composition of tumours from participants in the OVHIPEC-1 trial.
Methods: Whole-transcriptome RNA sequencing data were retrieved from high-grade serous ovarian cancer (HGSOC) samples from 147 patients obtained during interval CRS. We performed differential gene expression analysis and applied deconvolution methods to estimate cell-type proportions in bulk mRNA data, validated by histological assessment. We tested the interaction between treatment and potential predictors on progression-free survival using Cox proportional hazards models.
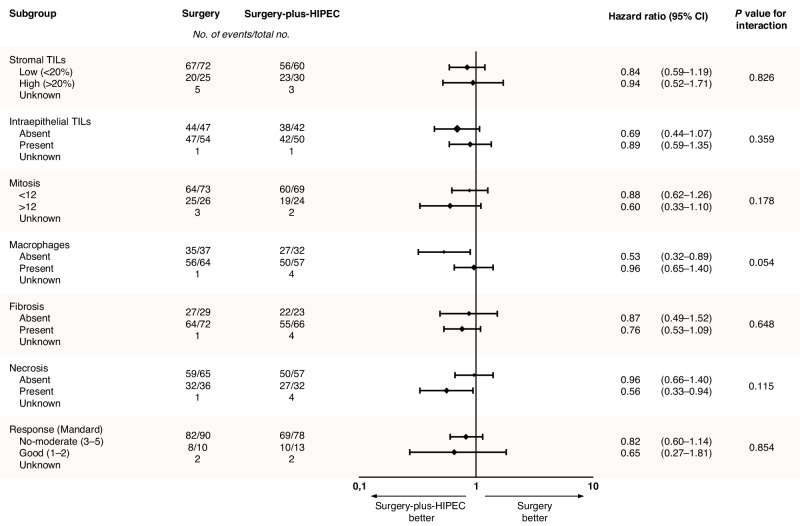
Results: While differential gene expression analysis did not yield any predictive biomarkers, the cellular composition, as characterised by deconvolution, indicated that the absence of macrophages and the presence of B cells in the tumour microenvironment are potential predictors of HIPEC benefit. The histological assessment confirmed the predictive value of macrophage absence.
Conclusion: Immune cell composition, in particular macrophages absence, may predict response to HIPEC in HGSOC and these hypothesis-generating findings warrant further investigation.
Clinical trial registration: NCT00426257.
© 2024. The Author(s), under exclusive licence to Springer Nature Limited.
Conflict of interest statement
KKVdV has served on advisory boards for Exact Sciences and AstraZeneca. HMH received honoraria from Roche Diagnostics BV. GSS has received institutional research support from Merck Sharp & Dohme, Agendia, AstraZeneca, Roche, and Novartis, and consulting fees from Biovica and Seagen. KH is a former employee at the Netherlands Cancer Institute and is currently working for Roche, Pharmaceutical Sciences, Basel, Switzerland. The research for this project was conducted in her position of researcher at the NKI. The remaining authors declare no competing interests.
Figures





References
-
- Aronson SL, Lopez-Yurda M, Koole SN, Schagen van Leeuwen JH, Schreuder HWR, Hermans RHM, et al. Cytoreductive surgery with or without hyperthermic intraperitoneal chemotherapy in patients with advanced ovarian cancer (OVHIPEC-1): final survival analysis of a randomised, controlled, phase 3 trial. Lancet Oncol. 2023;24:1109–18. 10.1016/S1470-2045(23)00396-0 - DOI - PubMed
-
- National Comprehensive Cancer Network. Ovarian Cancer (Version 3.2022) [Available from: https://www.nccn.org/login?ReturnURL=https://www.nccn.org/professionals/....
