

Prediction of cerebral infarction after bypass surgery in adult moyamoya disease: using pulsatility index on TCD
- PMID: 38867178
- PMCID: PMC11167940
- DOI: 10.1186/s12883-024-03707-y
Prediction of cerebral infarction after bypass surgery in adult moyamoya disease: using pulsatility index on TCD
Abstract
Background: At present, the most effective treatment for symptomatic moyamoya disease (MMD) is surgery. However, the high incidence of postoperative complications is a serious problem plaguing the surgical treatment of MMD, especially the acute cerebral infarction. Decreased cerebrovascular reserve is an independent risk factor for ischemic infarction, and the pulsatility index (PI) of transcranial Doppler (TCD) is a common intuitive index for evaluating intracranial vascular compliance. However, the relationship between PI and the occurrence of ischemic stroke after operation is unclear.
Objective: To explore whether the PI in the middle cerebral artery (MCA) could serve as a potential predictor for the occurrence of ischemic infarction after bypass surgery in MMD.
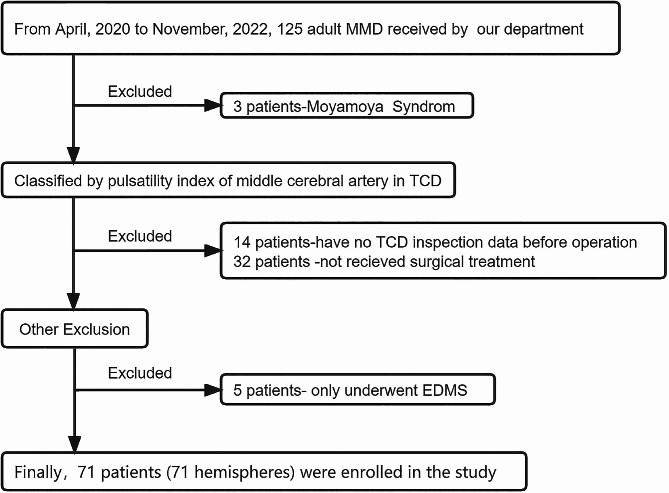
Methods: We performed a retrospective analysis of data from 71 patients who underwent combined revascularization surgery, including superficial temporal artery-middle cerebral artery (STA-MCA) anastomosis and encephalo-duro-myo-synangiosis (EDMS). The patients were divided into two groups according to the median of ipsilateral MCA-PI before operation, low PI group (MCA-PI < 0.614) and high PI group (MCA-PI ≥ 0.614). Univariate and multivariate regression analysis were used to explore risk factors affecting the occurrence of postoperative cerebral infarction.
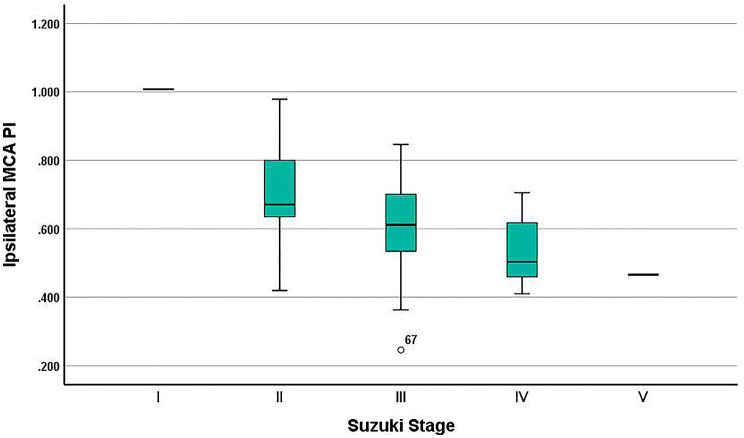
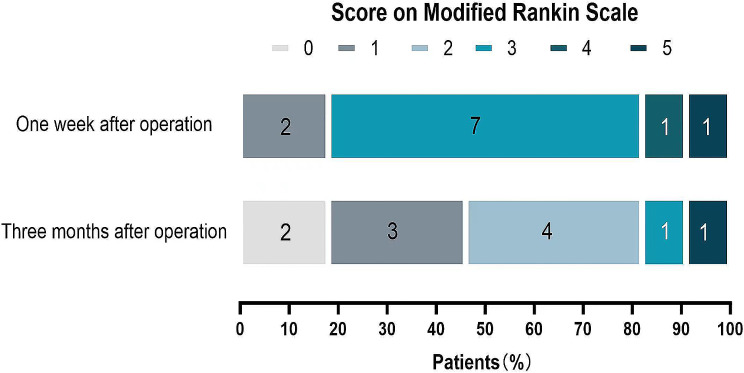
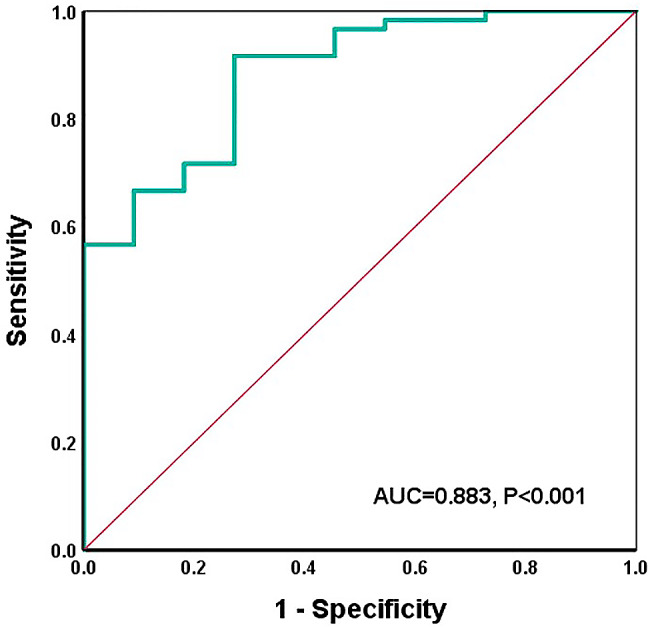
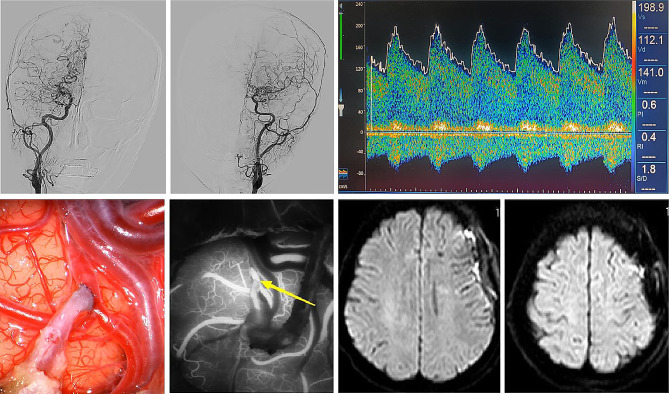
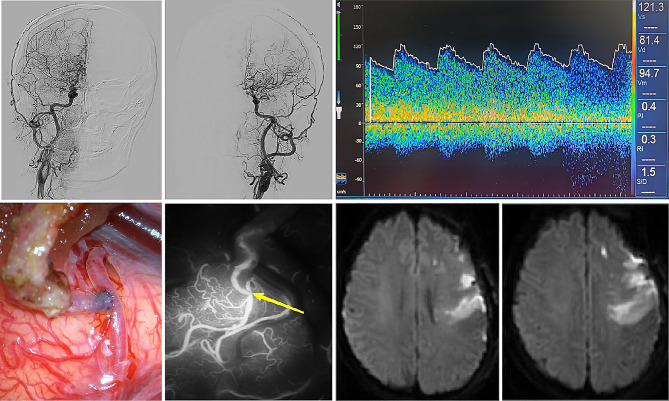
Results: Among the 71 patients with moyamoya disease, 11 patients had cerebral infarction within one week after revascularization. Among them, 10 patients' ipsilateral MCA-PI were less than 0.614, and another one's MCA- PI is higher than 0.614. Univariate analysis showed that the lower ipsilateral MCA-PI (0.448 ± 0.109 vs. 0.637 ± 0.124; P = 0.001) and higher Suzuki stage (P = 0.025) were linked to postoperative cerebral infarction. Multivariate analysis revealed that lower ipsilateral MCA-PI was an independent risk factor for predicting postoperative cerebral infarction (adjusted OR = 14.063; 95% CI = 6.265 ~ 37.308; P = 0.009).
Conclusions: A lower PI in the ipsilateral MCA may predict the cerebral infarction after combined revascularization surgery with high specificity. And combined revascularization appears to be safer for the moyamoya patients in early stages.
Keywords: Adult moyamoya disease; Infarction; PI; TCD.
© 2024. The Author(s).
Conflict of interest statement
The author declares that there is no conflict of interest in the materials or methods used in this study or the findings in this paper.
Figures
Similar articles
-
Prediction of cerebral infarction after bypass surgery in adult moyamoya disease: combing parameters on 4D perfusion CT with clinical related factors.Acta Neurochir (Wien). 2024 Nov 28;166(1):484. doi: 10.1007/s00701-024-06373-8. Acta Neurochir (Wien). 2024. PMID: 39607649 Free PMC article.
-
Incidence and Risk Factors of the Watershed Shift Phenomenon after Superficial Temporal Artery-Middle Cerebral Artery Anastomosis for Adult Moyamoya Disease.Cerebrovasc Dis. 2019;47(3-4):178-187. doi: 10.1159/000500802. Epub 2019 May 23. Cerebrovasc Dis. 2019. PMID: 31121577
-
Low flow velocity in the middle cerebral artery predicting infarction after bypass surgery in adult moyamoya disease.J Neurosurg. 2017 May;126(5):1573-1577. doi: 10.3171/2016.3.JNS152256. Epub 2016 Jun 3. J Neurosurg. 2017. PMID: 27257840
-
Treatment of moyamoya disease with intracranial aneurysm by surgical clipping combined with encephalo-duro-myo-synangiosis surgery: a case report and literature review.Int J Neurosci. 2024 Oct;134(10):1068-1074. doi: 10.1080/00207454.2023.2211729. Epub 2023 Jun 18. Int J Neurosci. 2024. PMID: 37330700 Review.
-
[History and Current Status of Direct or Combined Revascularization Surgery for Moyamoya Disease].No Shinkei Geka. 2025 May;53(3):514-521. doi: 10.11477/mf.030126030530030514. No Shinkei Geka. 2025. PMID: 40438014 Review. Japanese.
References
-
- Kazumata K, Ito M, Tokairin K, Ito Y, Houkin K, Nakayama N, Kuroda S, Ishikawa T, Kamiyama H. The frequency of postoperative stroke in moyamoya disease following combined revascularization: a single-university series and systematic review. J Neurosurg. 2014;121(2):432–40. doi: 10.3171/2014.1.JNS13946. - DOI - PubMed
MeSH terms
Grants and funding
- ZX2019-03-05/Yunnan Clinical Medical Center of Nervous System Diseases
- ZX2019-03-05/Yunnan Clinical Medical Center of Nervous System Diseases
- ZX2019-03-05/Yunnan Clinical Medical Center of Nervous System Diseases
- ZX2019-03-05/Yunnan Clinical Medical Center of Nervous System Diseases
- ZX2019-03-05/Yunnan Clinical Medical Center of Nervous System Diseases
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
