

Prevalence and associated risk factors for noma in Nigerian children: a systematic review and meta-analysis
- PMID: 38867180
- PMCID: PMC11170919
- DOI: 10.1186/s12903-024-04451-y
Prevalence and associated risk factors for noma in Nigerian children: a systematic review and meta-analysis
Abstract
Objectives: To determine the prevalence, case-fatality rate, and associated risk-factors of Noma in children in Nigeria.
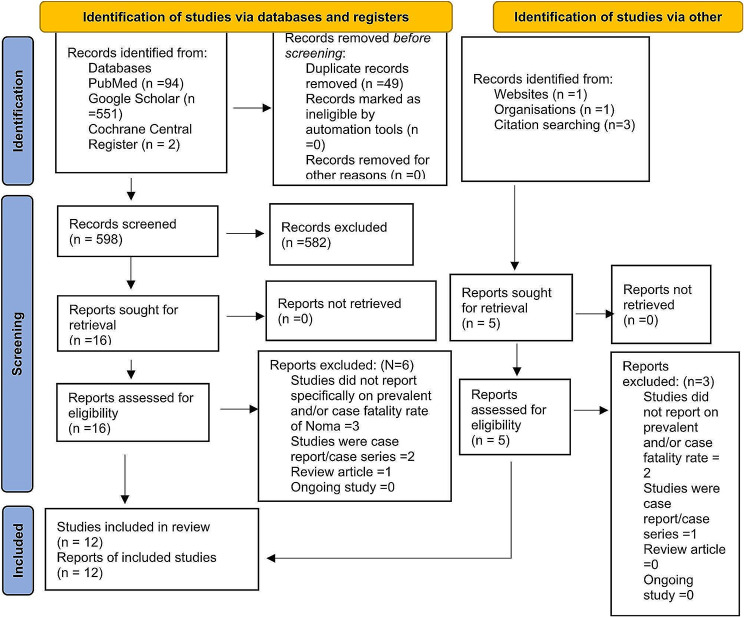
Methods: Search was conducted in PubMed, Google Scholar, and Cochrane Library databases. Data were extraction using a double-blind approach. Discrepancies were resolved by a third reviewer. Heterogeneity was evaluated using I2 statistics. Random-effects model was used for the meta-analysis and subgroup analysis was conducted. The study quality was evaluated using standard Critical-Appraisal-Checklist.
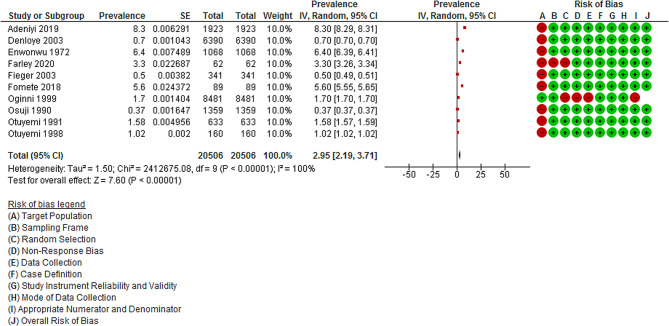
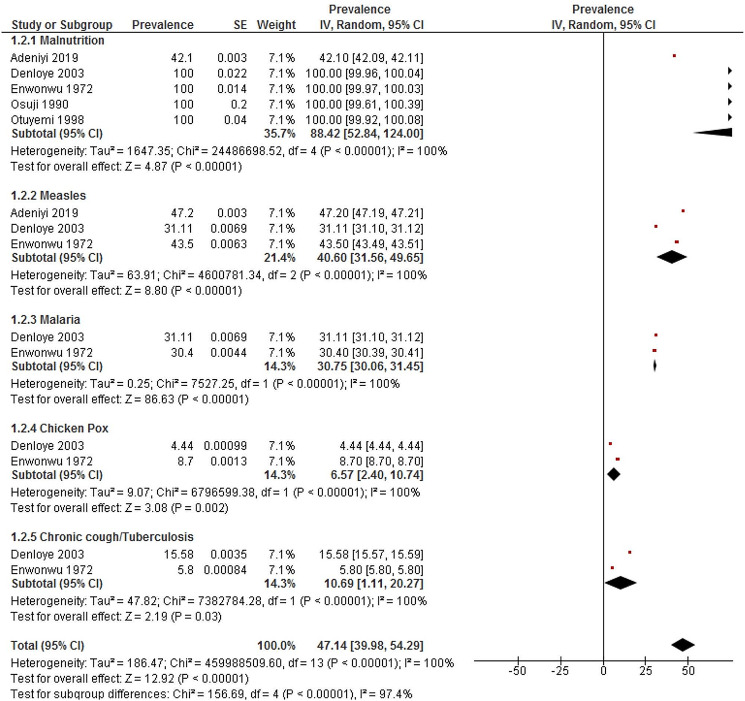
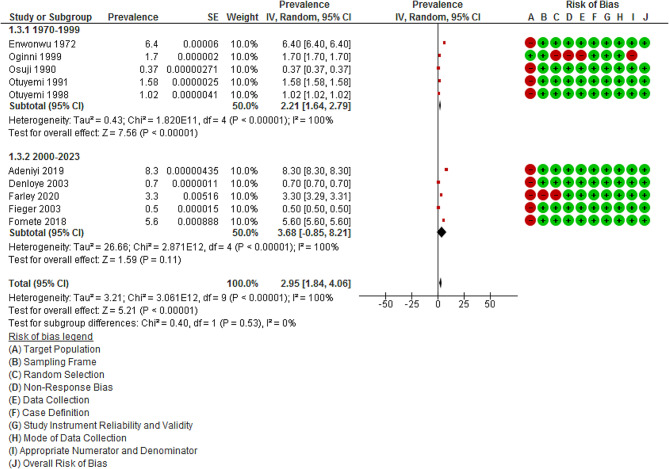
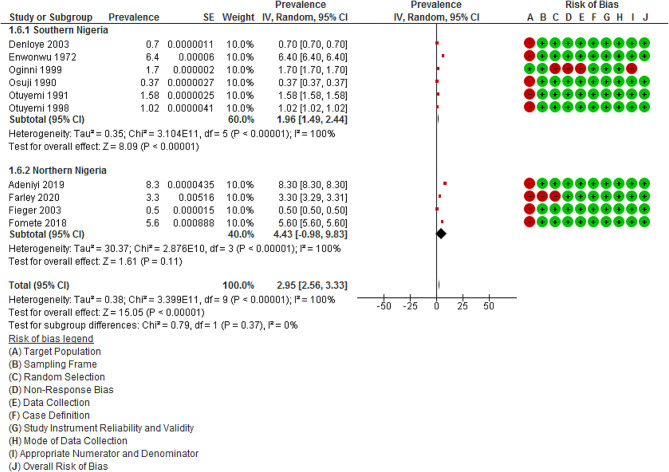
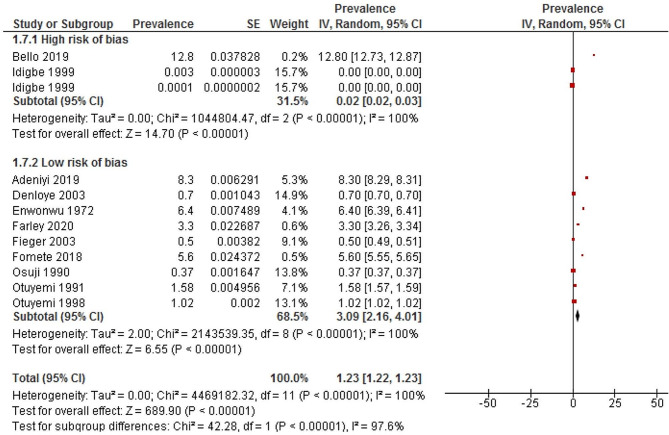
Results: Of the 1652 articles identified, 12 studies that met the inclusion criteria included 871 cases of Noma. Two studies had high-risk of bias and were excluded in the meta-analysis. Pooled prevalence of Noma was 2.95% (95%CI:2.19-3.71; Z = 7.60; p < 0.00001, I2:100.0). Case fatality was reported in one study. Sex-distribution had a male-to-female ratio of 1.1:1. Malnutrition (88.42%, 95%CI:52.84-124.00; I2:100.0), measles (40.60%; 95% CI:31.56-49.65; I2:100.0) and malaria (30.75%; 95% CI:30.06-31.45; I2:100.0) were the most notable associated risk-factors. Prevalence of Noma was non-significantly lower in southern (1.96%,95%CI:1.49-2.44;6 studies) than in northern (4.43%; 95%CI:-0.98-9.83; 4 studies) Nigeria. One study reported the prevalence of Noma in children younger than 5 years.
Conclusions: About every 3 in 100 children in Nigeria had Noma and the prevalence was non-significantly higher in northern than southern Nigeria. Malnutrition, measles, and malaria were major associated risk-factors. Case-fatality rate and prevalence based on different age-groups were inconclusive.
Keywords: Cancrum oris; Case fatality rate; Malaria; Malnutrition; Measles; Nigeria; Stomatitis gangrenosa.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

Similar articles
-
Pattern of noma (cancrum oris) and its risk factors in Northwestern Nigeria: A hospital-based retrospective study.Ann Afr Med. 2019 Jan-Mar;18(1):17-22. doi: 10.4103/aam.aam_5_18. Ann Afr Med. 2019. PMID: 30729928 Free PMC article.
-
An estimation of the incidence of noma in north-west Nigeria.Trop Med Int Health. 2003 May;8(5):402-7. doi: 10.1046/j.1365-3156.2003.01036.x. Trop Med Int Health. 2003. PMID: 12753633
-
Risk factors for diagnosed noma in northwest Nigeria: A case-control study, 2017.PLoS Negl Trop Dis. 2018 Aug 23;12(8):e0006631. doi: 10.1371/journal.pntd.0006631. eCollection 2018 Aug. PLoS Negl Trop Dis. 2018. PMID: 30138374 Free PMC article.
-
A review of noma cases in a tertiary hospital located in a conflict endemic region in Nigeria.Med Confl Surviv. 2022 Dec;38(4):295-306. doi: 10.1080/13623699.2022.2114121. Epub 2022 Aug 24. Med Confl Surviv. 2022. PMID: 36003023 Review.
-
Infectious oral necrosis (cancrum oris) in Nigerian children: a review.Community Dent Oral Epidemiol. 1985 Jun;13(3):190-4. doi: 10.1111/j.1600-0528.1985.tb00443.x. Community Dent Oral Epidemiol. 1985. PMID: 2861938 Review.
Cited by
-
Resurgence of Noma (Cancrum Oris) in Nigeria.Am J Trop Med Hyg. 2024 Sep 24;111(6):1164-1165. doi: 10.4269/ajtmh.24-0406. Print 2024 Dec 4. Am J Trop Med Hyg. 2024. PMID: 39317183
References
-
- Tovani-Palone MR. Noma as a neglected tropical disease: coordinated actions are needed. Eur Arch Paediatr Dent. 2024 Feb;26. 10.1007/s40368-024-00872-z. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
