

Association between the atherogenic index of plasma and left ventricular hypertrophy in patients with obstructive sleep apnea: a retrospective cross-sectional study
- PMID: 38867215
- PMCID: PMC11167813
- DOI: 10.1186/s12944-024-02170-5
Association between the atherogenic index of plasma and left ventricular hypertrophy in patients with obstructive sleep apnea: a retrospective cross-sectional study
Abstract
Background: The atherogenic index of plasma (AIP) is a simple and reliable marker of insulin resistance and is closely associated with various cardiovascular diseases (CVDs). However, the relationships between AIP and left ventricular (LV) geometric indicators have not been adequately assessed. This study was carried out to investigate the association between AIP and LV geometric abnormalities in obstructive sleep apnea (OSA) patients.
Methods: This retrospective cross-sectional study included a total of 618 OSA patients (57.3 ± 12.4 years, 73.1% males, BMI 28.1 ± 4.2 kg/m2) who underwent echocardiography. Patients with OSA were diagnosed with clinical symptoms and an apnea-hypopnea index ≥ 5.0. LV hypertrophy (LVH) was defined as left ventricular mass index (LVMIh2.7) ≥ 50.0 g/m2.7 for men and 47.0 g/m2.7 for women. AIP was calculated as log10 (TG/HDL-C).
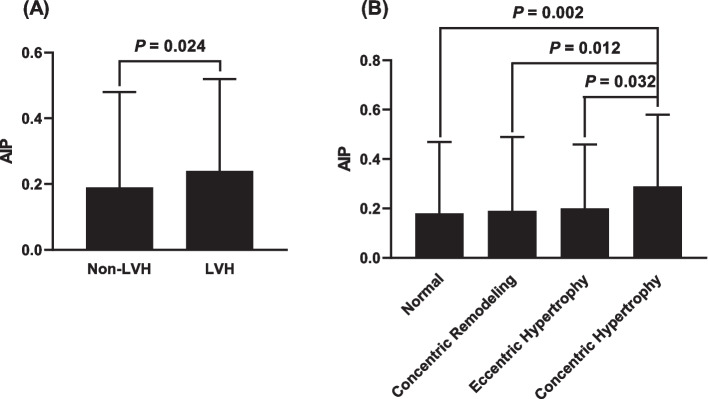
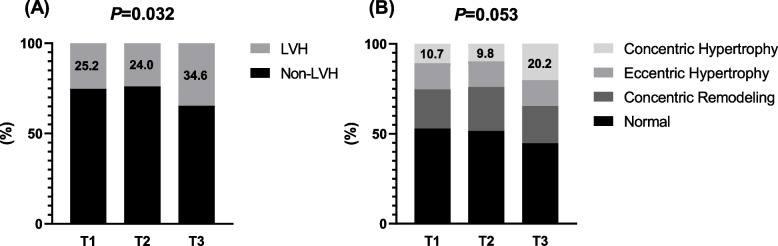
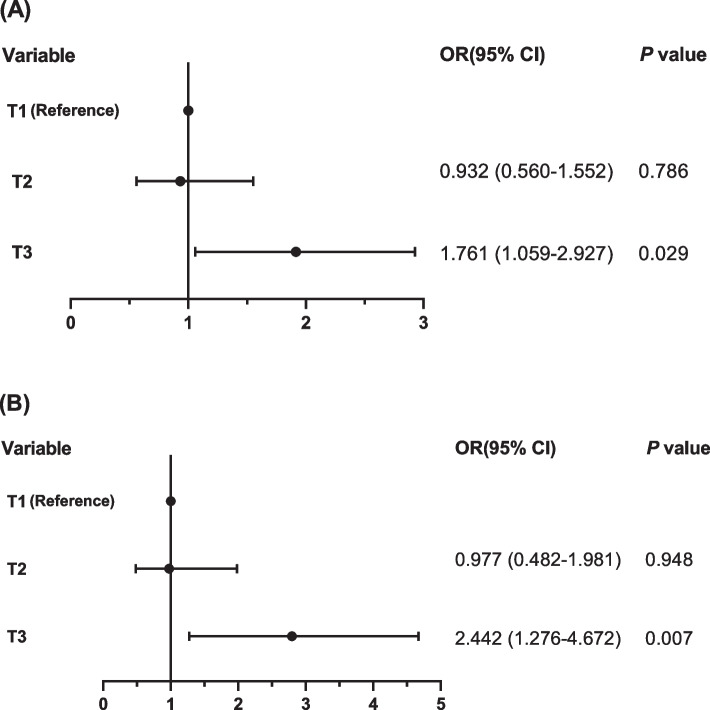
Results: Compared with the non-LVH group, AIP was significantly higher in the LVH group (0.19 ± 0.29 vs 0.24 ± 0.28, P = 0.024) and the concentric LVH group (0.18 ± 0.29, 0.19 ± 0.30, 0.20 ± 0.26 and 0.29 ± 0.29 in the control, concentric remodeling, eccentric hypertrophy and concentric hypertrophy groups, respectively, P = 0.021). Meanwhile, in the group of patients with the highest AIP tertile, the levels of LVMIh2.7 (42.8 ± 10.5, 43.2 ± 9.3 and 46.1 ± 12.1 in the T1, T2 and T3 groups, respectively, P = 0.003), and the prevalence of LVH (25.2%, 24.0% and 34.6% in the T1, T2 and T3 groups, respectively, P = 0.032) and concentric LVH (10.7%, 9.8% and 20.2% in the T1, T2 and T3 groups, respectively, P = 0.053) were higher compared with those in the other groups. Positive correlations between AIP and LV geometric indicators including the LVMIh2.7, LVMIBSA, LV mass (LVM), diastolic left ventricular inner diameter (LVIDd), diastolic left ventricular posterior wall thickness (PWTd) and diastolic interventricular septal thickness (IVSTd), were revealed according to correlation analysis (P < 0.05). Furthermore, AIP was independently associated with LVMIh2.7 according to multivariate linear regression model (β = 0.125, P = 0.001). Notably, AIP remained independently associated with an elevated risk of LVH [odds ratio (OR) = 1.317 per 1 standard deviation (SD) increment, 95% confidence interval (CI): 1.058 - 1.639, P = 0.014) and concentric LVH (OR = 1.545 per 1 SD increment, 95% CI: 1.173 - 2.035, P = 0.002) after fully adjusting for all confounding risk factors by multivariate logistic regression analyses.
Conclusions: AIP was independently associated with an increased risk of LVH and concentric LVH in OSA patients. Therefore, AIP, as a practical and cost-effective test, might be useful in monitoring hypertrophic remodeling of the heart and improving CVDs risk stratification in clinical management of OSA.
Keywords: Atherogenic index of plasma; Insulin resistance; Left ventricular hypertrophy; Obstructive sleep apnea.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Targeting Concentric Left Ventricular Hypertrophy in Obstructive Sleep Apnea Syndrome. A Meta-analysis of Echocardiographic Studies.Am J Hypertens. 2020 Apr 1;33(4):310-315. doi: 10.1093/ajh/hpz198. Am J Hypertens. 2020. PMID: 31863113
-
The association of sleep disordered breathing with left ventricular remodeling in CAD patients: a cross-sectional study.BMC Cardiovasc Disord. 2017 Sep 18;17(1):250. doi: 10.1186/s12872-017-0684-1. BMC Cardiovasc Disord. 2017. PMID: 28923022 Free PMC article.
-
Gender-specific contribution of cardiometabolic index and lipid accumulation product to left ventricular geometry change in general population of rural China.BMC Cardiovasc Disord. 2018 Apr 10;18(1):62. doi: 10.1186/s12872-018-0798-0. BMC Cardiovasc Disord. 2018. PMID: 29631555 Free PMC article.
-
Severe obstructive sleep apnea elicits concentric left ventricular geometry.J Hypertens. 2010 May;28(5):1074-82. doi: 10.1097/hjh.0b013e328336c90a. J Hypertens. 2010. PMID: 20411620
-
Obstructive sleep apnoea syndrome and left ventricular hypertrophy: a meta-analysis of echocardiographic studies.J Hypertens. 2020 Sep;38(9):1640-1649. doi: 10.1097/HJH.0000000000002435. J Hypertens. 2020. PMID: 32371766
Cited by
-
Atherogenic index of plasma and obesity-related risk of stroke in middle-aged and older Chinese adults: a national prospective cohort study.Diabetol Metab Syndr. 2024 Oct 8;16(1):245. doi: 10.1186/s13098-024-01481-y. Diabetol Metab Syndr. 2024. PMID: 39380102 Free PMC article.
-
Prediction of early myocardial damage in obstructive sleep apnea patients using combined logistic regression and QUEST decision tree models.Braz J Med Biol Res. 2025 Jun 20;58:e14757. doi: 10.1590/1414-431X2025e14757. eCollection 2025. Braz J Med Biol Res. 2025. PMID: 40561277 Free PMC article.
-
Prognostic value of atherogenic index of plasma in pulmonary hypertension.Front Med (Lausanne). 2025 Jan 13;11:1490695. doi: 10.3389/fmed.2024.1490695. eCollection 2024. Front Med (Lausanne). 2025. PMID: 39871832 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
