

Clinical Results of Primary Repair Versus Reconstruction of the Anterior Cruciate Ligament: A Systematic Review and Meta-analysis of Contemporary Trials
- PMID: 38867918
- PMCID: PMC11168252
- DOI: 10.1177/23259671241253591
Clinical Results of Primary Repair Versus Reconstruction of the Anterior Cruciate Ligament: A Systematic Review and Meta-analysis of Contemporary Trials
Abstract
Background: Primary anterior cruciate ligament (ACL) repair has gained renewed interest in select centers for patients with proximal or midsubstance ACL tears. Therefore, it is important to reassess contemporary clinical outcomes of ACL repair to determine whether a clinical benefit exists over the gold standard of ACL reconstruction (ACLR).
Purpose: To (1) perform a meta-analysis of comparative trials to determine whether differences in clinical outcomes and adverse events exist between ACL repair versus ACLR and (2) synthesize the midterm outcomes of available trials.
Study design: Systematic review; Level of evidence, 3.
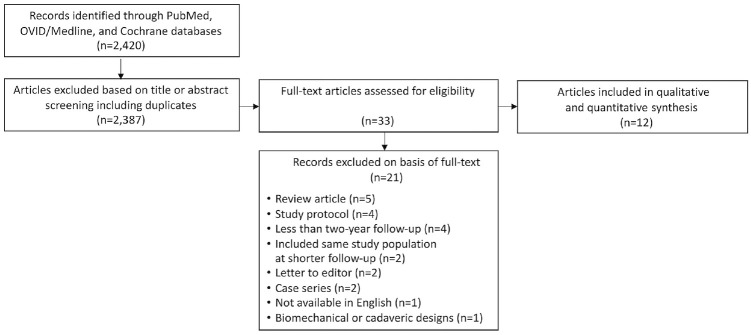
Methods: The PubMed, OVID/Medline, and Cochrane databases were queried in August 2023 for prospective and retrospective clinical trials comparing ACL repair and ACLR. Data pertaining to tear location, surgical technique, adverse events, and clinical outcome measures were recorded. DerSimonian-Laird random-effects models were constructed to quantitatively evaluate the association between ACL repair/ACLR, adverse events, and clinical outcomes. A subanalysis of minimum 5-year outcomes was performed.
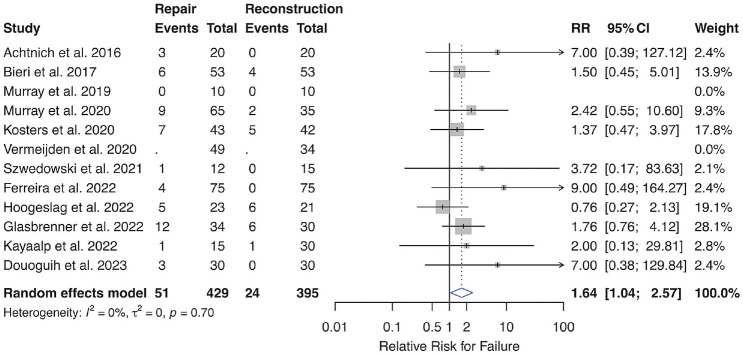
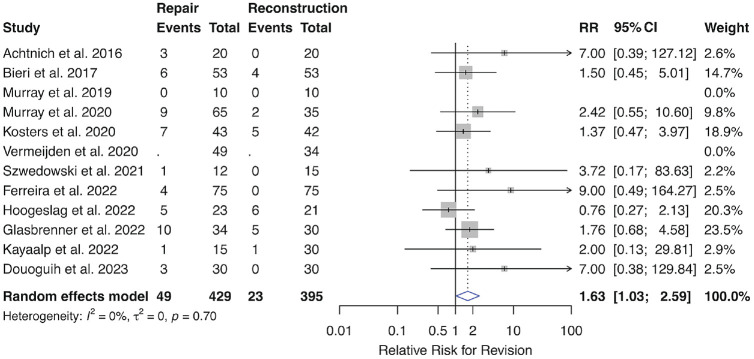
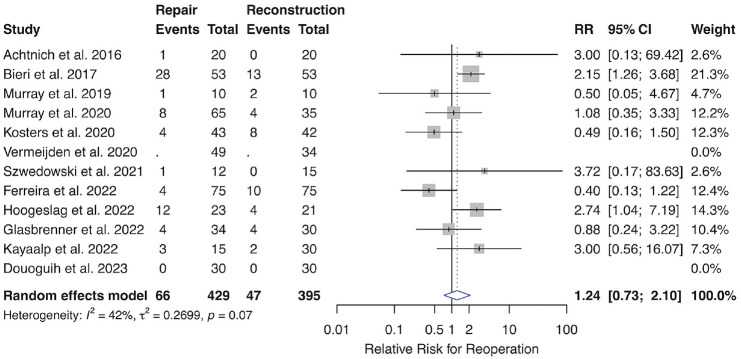
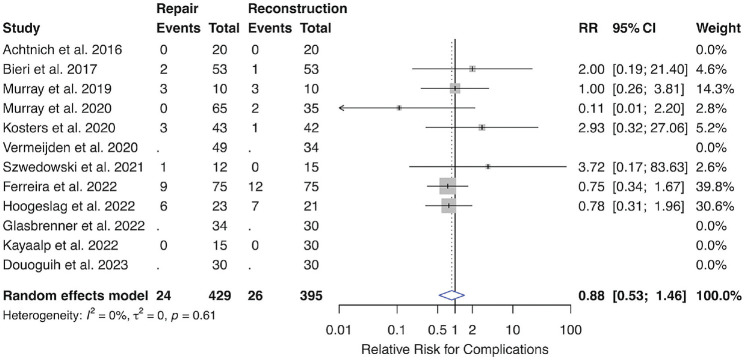
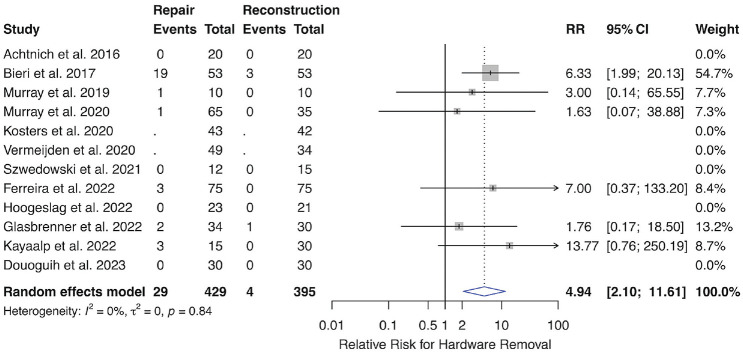
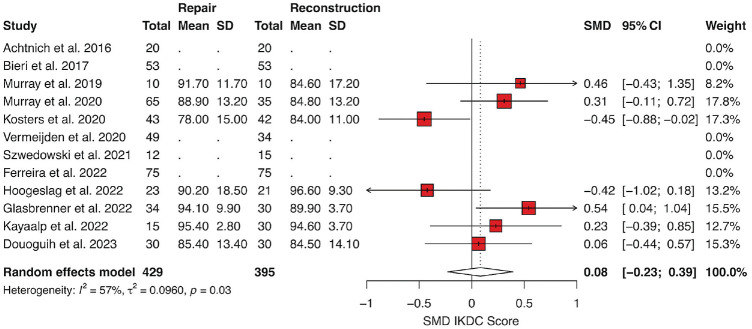
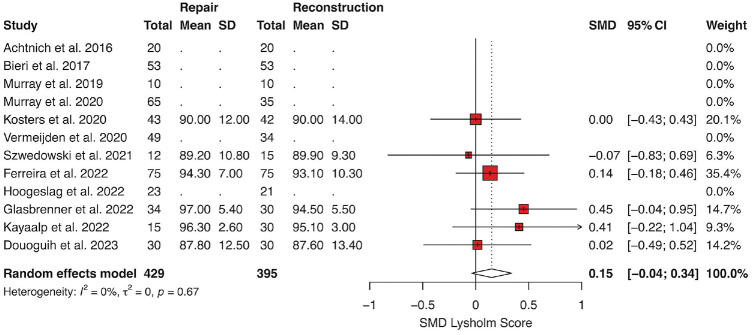
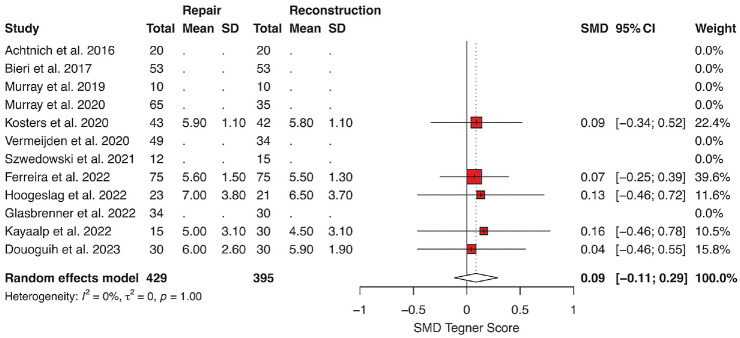
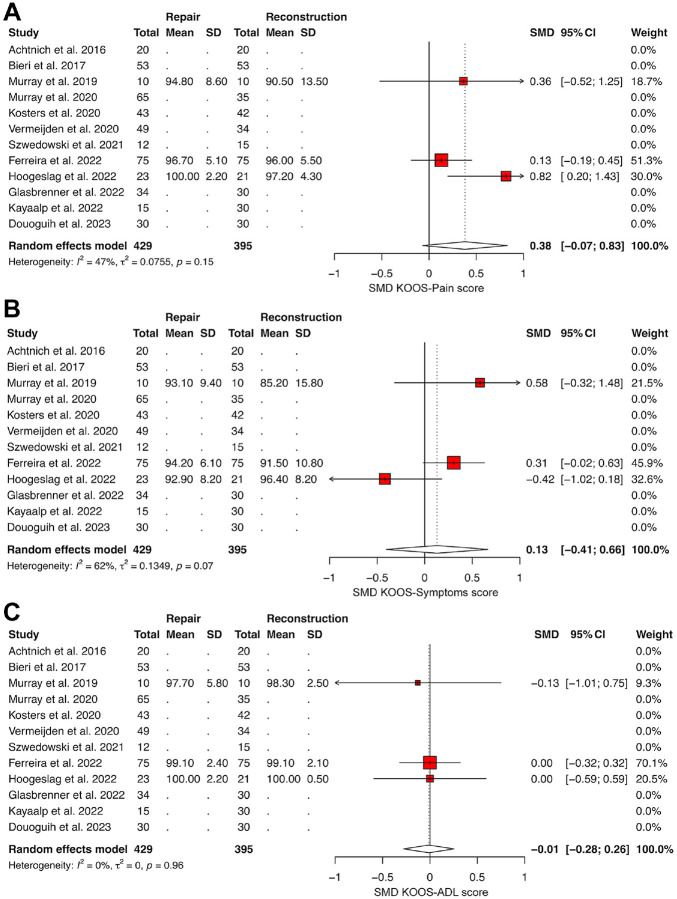
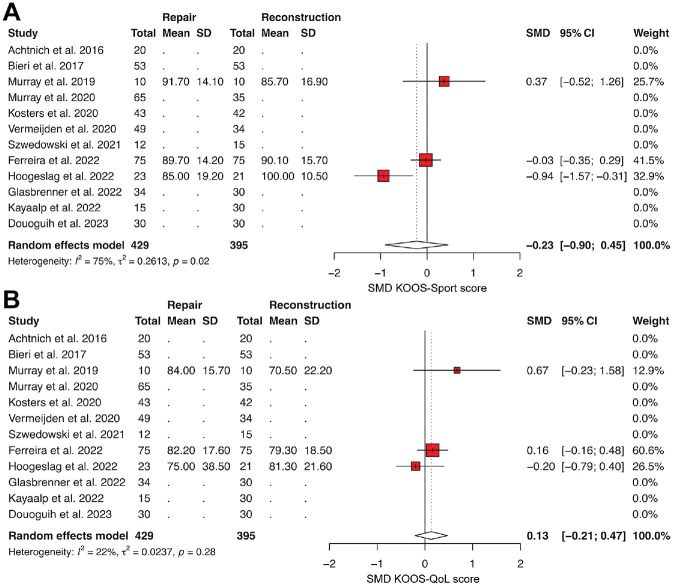
Results: Twelve studies (893 patients; 464 ACLR and 429 ACL repair) were included. Random-effects models demonstrated a higher relative risk (RR) of recurrent instability/clinical failure (RR = 1.64; 95% confidence interval [CI], 1.04-2.57; P = .032), revision ACLR (RR = 1.63; 95% CI, 1.03-2.59; P = .039), and hardware removal (RR = 4.94; 95% CI, 2.10-11.61; P = .0003) in patients who underwent primary ACL repair versus ACLR. The RR of reoperations and complications (knee-related) were not significantly different between groups. No significant differences were observed when comparing patient-reported outcome scores. In studies with minimum 5-year outcomes, no significant differences in adverse events or Lysholm scores were observed.
Conclusion: In contemporary comparative trials of ACL repair versus ACLR, the RR of clinical failure, revision surgery due to ACL rerupture, and hardware removal was greater for primary ACL repair compared with ACLR. There were no observed differences in patient-reported outcome scores, reoperations, or knee-related complications between approaches. In the limited literature reporting on minimum 5-year outcomes, significant differences in adverse events or the International Knee Documentation Committee score were not observed.
Keywords: adverse events; anterior cruciate ligament; patient-reported outcomes; reconstruction; repair.
© The Author(s) 2024.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: A.P. has received education payments from Smith+Nephew and hospitality payments from Medical Device Business Services. B.U.N. has received grant support from Arthrex, education payments from Arthrex and Smith+Nephew, consulting fees from Stryker, and hospitality payments from Medical Device Business Services and Zimmer Biomet. A.S.R. has received education payments from Gotham Surgical; consulting fees from Anika Therapeutics, Bodycad, Smith+Nephew, Xiros, Stryker, Flexion Therapeutics, Arthrex, and Heron Therapeutics; and nonconsulting fees from Arthrex and Smith+Nephew. A.S.P. has received consulting fees from Smith+ Nephew, Zimmer Biomet, DePuy Synthes, Exactech, and Stryker; nonconsulting fees from Smith+Nephew; royalties from Smith+Nephew and Zimmer Biomet; and has stock/stock options in Smith+Nephew. B.T.K. has received education payments from Arthrex; consulting fees from Arthrex; nonconsulting fees from Arthrex and Synthes; royalties from Arthrex; and hospitality payments from Stryker and Smith+Nephew. R.J.W. has received royalty or license from Arthrex; consulting fees and nonconsulting fees from Arthrex; and has stock/stock options in Smith+Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
-
- Achtnich A, Herbst E, Forkel P, et al. Acute proximal anterior cruciate ligament tears: outcomes after arthroscopic suture anchor repair versus anatomic single-bundle reconstruction. Arthroscopy. 2016;32(12):2562-2569. - PubMed
-
- Ahmad SS, Schreiner AJ, Hirschmann MT, et al. Dynamic intraligamentary stabilization for ACL repair: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2019;27(1):13-20. - PubMed
-
- Bieri KS, Scholz SM, Kohl S, Aghayev E, Staub LP. Dynamic intraligamentary stabilization versus conventional ACL reconstruction: a matched study on return to work. Injury. 2017;48(6):1243-1248. - PubMed
-
- De Smet E, Heusdens CHW, Parizel PM, Van Dyck P. MRI following primary repair of the anterior cruciate ligament. Clin Radiol. 2019;74(8):649.e1-649.e10. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
