

doi: 10.1002/imt2.108.
eCollection 2023 Aug.
The salivary microbiota is altered in cervical dysplasia patients and influenced by conization
Affiliations
- PMID: 38867925
- PMCID: PMC10989756
- DOI: 10.1002/imt2.108
Item in Clipboard
The salivary microbiota is altered in cervical dysplasia patients and influenced by conization
Imeta.
.
Abstract
This study supports the correlation between the salivary microbiota and cervical dysplasia and suggests that smoking influences the salivary microbiota.
© 2023 The Authors. iMeta published by John Wiley & Sons Australia, Ltd on behalf of iMeta Science.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

The study design and the comparison of salivary microbial alpha diversity, beta diversity, salivary genera, and bacterial functions of all the participants. (A) The study design and comparison groups. This cross‐sectional study recruited 20 healthy volunteers who visited for a routine dental examination at a dental clinic and 47 participants who visited for a vaginal examination at Karolinska University Hospital. Among these 47 women, 28 visited due to potential dysplasia, 19 of whom were treated with conization after being diagnosed with a high‐grade squamous intraepithelial lesion (HSIL). Histological data showed that 8 women had low‐grade squamous intraepithelial lesion (LSIL), 19 had HSIL, and 20 were within normal limits (WNL). We grouped individuals with WNL as a group without dysplasia and LSIL combined with HSIL as the dysplasia group. In addition, 24 of 28 participants, who came for checking potential dysplasia and confirmed with dysplasia, were identified as the predysplasia (+) group. The 16 of the 19 participants who visited for a follow‐up examination after conization treatment and confirmed dysplasia‐free were grouped into the postdysplasia (−) group. (B) The Shannon index was compared among participants with and without cervical dysplasia, as well as the participants who visited for the dental examination (control group). (C) The Shannon index was compared among patients from the predysplasia (+) and postdysplasia (−) groups and participants from the control group. The Kruskal–Wallis test and the Tukey–Kramer post hoc test were used to test microbial alpha diversity differences between more than two groups. False discovery rate (FDR) < 0.05 **FDR < 0.01, ***FDR < 0.001. (D) The salivary microbial beta diversity (nonmetric multidimensional scaling [NMDS] analysis with amplicon sequence variants [ASVs] based on Bray–Curtis distance matrices and ANOSIM analysis) was compared among participants with and without cervical dysplasia and from the control group. (E) The salivary microbial beta diversity was compared among patients from the predysplasia (+) and postdysplasia (−) groups and participants from the control group. (F) The significantly changed salivary microbiota genera from the comparison among participants with and without cervical dysplasia and the control group. (G) The significantly changed salivary microbiota genera from the comparison among patients from the predysplasia (+) and postdysplasia (−) groups and participants from the control group. (H) The significantly changed salivary microbiota predicted immune‐related functions from the comparison among participants with and without cervical dysplasia and the control group. FDR < 0.05, **FDR < 0.01, ***FDR < 0.001. (I) The correlation between differential salivary bacterial functions and the 30 most abundant genera based on the data from all 67 participants. The differential salivary bacterial functions were identified from the comparison between participants with and without cervical dysplasia and the control group. The Kruskal–Wallis test with the Tukey–Kramer post hoc test was used to test for differences in microbial genera and function. For correlation analysis, only Spearman's rank correlation coefficient greater than 0.4 and a FDR less than 0.05 are presented. The blue grid indicates a positive correlation, and the red grid indicates a negative correlation. ***FDR < 0.001.
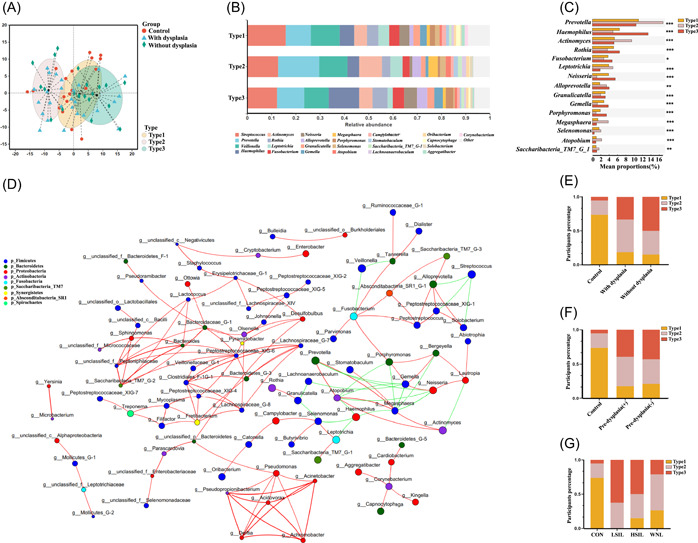
Salivary microbial types of all the participants. (A) Three different salivary microbial types were identified based on the genera of salivary microbes. The partitioning around medoids (PAM) cluster based on the Jensen–Shannon distance (JSD) and the Calinski–Harabasz (CH) indices was used. (B) The comparison of microbial composition among three different salivary microbial types at the genus level. (C) The significantly altered genera among three different salivary microbial types. The Kruskal–Wallis test with the Tukey–Kramer post hoc test was used to test differences in the microbial genera. *FDR < 0.05, **FDR < 0.01, ***FDR < 0.001. (D) The correlation network among genera in salivary microbiota based on Spearman's rank correlation coefficient analysis. Only Spearman's rank correlation coefficient greater than 0.5 and a FDR less than 0.05 are presented. The red line represents a positive correlation, and the green line represents a negative correlation. (E) The distribution of different microbiota types among participants with and without cervical dysplasia and the control group. (F) The distribution of different microbiota types among patients from the predysplasia (+) and postdysplasia (–) groups and the control group. (G) The distribution of different microbiota types among participants from the control group and the LSIL, HSIL, and WNL groups.

Comparison of salivary microbial alpha diversity, beta diversity, salivary genera, and salivary bacterial functions between participants with and without cervical dysplasia and between participants from the predysplasia (+) and postdysplasia (−) groups. (A) The Shannon index was compared between the participants with and without cervical dysplasia. (B) The Shannon index was compared between the patients from the predysplasia (+) and postdysplasia (−) groups. The Mann–Whitney U test was carried out to compare the two groups. (C) The salivary microbial beta diversity was compared between the participants with and without cervical dysplasia. (D) The salivary microbial beta diversity was compared between the patients from the predysplasia (+) and postdysplasia (−) groups. (E) The significantly changed salivary microbiota genera from the comparison between participants with and without cervical dysplasia. *FDR < 0.05. (F) The significantly changed salivary microbiota genera from the comparison between patients from the predysplasia (+) and postdysplasia (−) groups. *FDR < 0.05. (G) The cosignificantly changed salivary microbiota predicted immune‐related functions from the comparison between patients with and without cervical dysplasia. *FDR < 0.05. (H) The correlation between the codifferential salivary bacterial functions and the 30 most abundant genera based on the data from the 47 vaginal examination participants. The differential salivary bacterial functions were identified from the comparison among participants with and without cervical dysplasia. The Mann–Whitney U test was carried out to compare the two groups. For correlation analysis, only Spearman's rank correlation coefficient greater than 0.4 and a false discovery rate (FDR) less than 0.05 are presented. The blue grid indicates a positive correlation, and the red grid indicates a negative correlation. **FDR < 0.01. (I–K) The area under the curve (AUC) of receiver operating characteristic (ROC) analyses helps to identify the diagnostic accuracy of participants with and without cervical dysplasia based on the salivary Actinomyces abundance (I), the conventional vaginal cytology and HR‐HPV testing (J), as well as the conventional vaginal cytology and HR‐HPV testing plus salivary Actinomyces abundance (K).
Similar articles
-
Predictive factors from cold knife conization for residual cervical intraepithelial neoplasia in subsequent hysterectomy.Am J Obstet Gynecol. 1995 Aug;173(2):361-6; discussion 366-8. doi: 10.1016/0002-9378(95)90253-8. Am J Obstet Gynecol. 1995. PMID: 7645609
-
Cold-knife conization versus the loop electrosurgical excision procedure for treatment of cervical dysplasia.Eur J Gynaecol Oncol. 2008;29(1):83-5. Eur J Gynaecol Oncol. 2008. PMID: 18386472
-
The pre- and postoperative value of endocervical curettage in the detection of cervical intraepithelial neoplasia and invasive cervical cancer.Gynecol Oncol. 1998 Oct;71(1):46-9. doi: 10.1006/gyno.1998.5120. Gynecol Oncol. 1998. PMID: 9784317
-
[Radical conization of intraepithelial neoplasia].Ugeskr Laeger. 2014 Apr 14;176(8):V10120605. Ugeskr Laeger. 2014. PMID: 25096463 Review. Danish.
-
Pregnancy Outcomes Following Cervical Conization or Loop Electrosurgical Excision Procedures.Obstet Gynecol Surv. 2017 Aug;72(8):494-499. doi: 10.1097/OGX.0000000000000468. Obstet Gynecol Surv. 2017. PMID: 28817166 Review.
References
-
- Canfell, Karen , Kim Jane J., Brisson Marc, Keane Adam, Simms Kate T., Caruana Michael, Burger Emily A., et al. 2020. “Mortality Impact Of Achieving WHO Cervical Cancer Elimination Targets: a Comparative Modelling Analysis in 78 Low‐Income and Lower‐Middle‐Income Countries.” The Lancet 395: 591–603. 10.1016/S0140-6736(20)30157-4 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources