

Scientific opinion on the tolerable upper intake level for iron
- PMID: 38868106
- PMCID: PMC11167337
- DOI: 10.2903/j.efsa.2024.8819
Scientific opinion on the tolerable upper intake level for iron
Abstract
Following a request from the European Commission, the EFSA Panel on Nutrition, Novel Foods and Food Allergens (NDA) was asked to deliver a scientific opinion on the tolerable upper intake level (UL) for iron. Systematic reviews were conducted to identify evidence regarding high iron intakes and risk of chronic diseases, adverse gastrointestinal effects and adverse effects of iron supplementation in infancy, young childhood and pregnancy. It is established that systemic iron overload leads to organ toxicity, but no UL could be established. The only indicator for which a dose-response could be established was black stools, which reflect the presence of large amounts of unabsorbed iron in the gut. This is a conservative endpoint among the chain of events that may lead to systemic iron overload but is not adverse per se. Based on interventions in which black stools did not occur at supplemental iron intakes of 20-25 mg/day (added to a background intake of 15 mg/day), a safe level of intake for iron of 40 mg/day for adults (including pregnant and lactating women) was established. Using allometric scaling (body weight0.75), this value was scaled down to children and adolescents and safe levels of intakes between 10 mg/day (1-3 years) and 35 mg/day (15-17 years) were derived. For infants 7-11 months of age who have a higher iron requirement than young children, allometric scaling was applied to the supplemental iron intakes (i.e. 25 mg/day) and resulted in a safe level of supplemental iron intake of 5 mg/day. This value was extended to 4-6 month-old infants and refers to iron intakes from fortified foods and food supplements, not from infant and follow-on formulae. The application of the safe level of intake is more limited than a UL because the intake level at which the risk of adverse effects starts to increase is not defined.
Keywords: adverse effects; iron homeostasis; iron overload; safe level of intake.
© 2024 European Food Safety Authority. EFSA Journal published by Wiley‐VCH GmbH on behalf of European Food Safety Authority.
Conflict of interest statement
If you wish to access the declaration of interests of any expert contributing to an EFSA scientific assessment, please contact interestmanagement@efsa.europa.eu.
Figures

Similar articles
-
Scientific opinion on the tolerable upper intake level for vitamin B6.EFSA J. 2023 May 17;21(5):e08006. doi: 10.2903/j.efsa.2023.8006. eCollection 2023 May. EFSA J. 2023. PMID: 37207271 Free PMC article.
-
Scientific opinion on the tolerable upper intake level for preformed vitamin A and β-carotene.EFSA J. 2024 Jun 6;22(6):e8814. doi: 10.2903/j.efsa.2024.8814. eCollection 2024 Jun. EFSA J. 2024. PMID: 38846679 Free PMC article.
-
Scientific opinion on the tolerable upper intake level for manganese.EFSA J. 2023 Dec 8;21(12):e8413. doi: 10.2903/j.efsa.2023.8413. eCollection 2023 Dec. EFSA J. 2023. PMID: 38075631 Free PMC article.
-
Safety and nutritional assessment of GM plants and derived food and feed: the role of animal feeding trials.Food Chem Toxicol. 2008 Mar;46 Suppl 1:S2-70. doi: 10.1016/j.fct.2008.02.008. Epub 2008 Feb 13. Food Chem Toxicol. 2008. PMID: 18328408 Review.
-
Perspective: Call for Re-evaluation of the Tolerable Upper Intake Level for Magnesium Supplementation in Adults.Adv Nutr. 2023 Sep;14(5):973-982. doi: 10.1016/j.advnut.2023.06.008. Epub 2023 Jul 22. Adv Nutr. 2023. PMID: 37487817 Free PMC article. Review.
Cited by
-
Assessment of genetically modified maize DP910521 (application GMFF-2021-2473).EFSA J. 2024 Aug 1;22(8):e8887. doi: 10.2903/j.efsa.2024.8887. eCollection 2024 Aug. EFSA J. 2024. PMID: 39099615 Free PMC article.
-
Peer review of the pesticide risk assessment of the active substance elemental iron.EFSA J. 2024 Oct 25;22(10):e9056. doi: 10.2903/j.efsa.2024.9056. eCollection 2024 Oct. EFSA J. 2024. PMID: 39463784 Free PMC article. Review.
-
Safety of soy leghemoglobin from genetically modified Komagataella phaffii as a food additive.EFSA J. 2024 Jun 28;22(6):e8822. doi: 10.2903/j.efsa.2024.8822. eCollection 2024 Jun. EFSA J. 2024. PMID: 38946918 Free PMC article.
-
Guidance for establishing and applying tolerable upper intake levels for vitamins and essential minerals.EFSA J. 2024 Nov 6;22(11):e9052. doi: 10.2903/j.efsa.2024.9052. eCollection 2024 Nov. EFSA J. 2024. PMID: 39507293 Free PMC article.
-
Approach to anaemia in gastrointestinal disease: A position paper by the ESPGHAN Gastroenterology Committee.J Pediatr Gastroenterol Nutr. 2025 Mar;80(3):510-532. doi: 10.1002/jpn3.12454. Epub 2025 Jan 9. J Pediatr Gastroenterol Nutr. 2025. PMID: 39783775 Free PMC article.
References
-
- Balder, H. F. , Vogel, J. , Jansen, M. C. , Weijenberg, M. P. , van den Brandt, P. A. , Westenbrink, S. , van der Meer, R. , & Goldbohm, R. A. (2006). Heme and chlorophyll intake and risk of colorectal cancer in The Netherlands cohort study. Cancer Epidemiology, Biomarkers & Prevention, 15, 717–725. 10.1158/1055-9965.EPI-05-0772 - DOI - PubMed
-
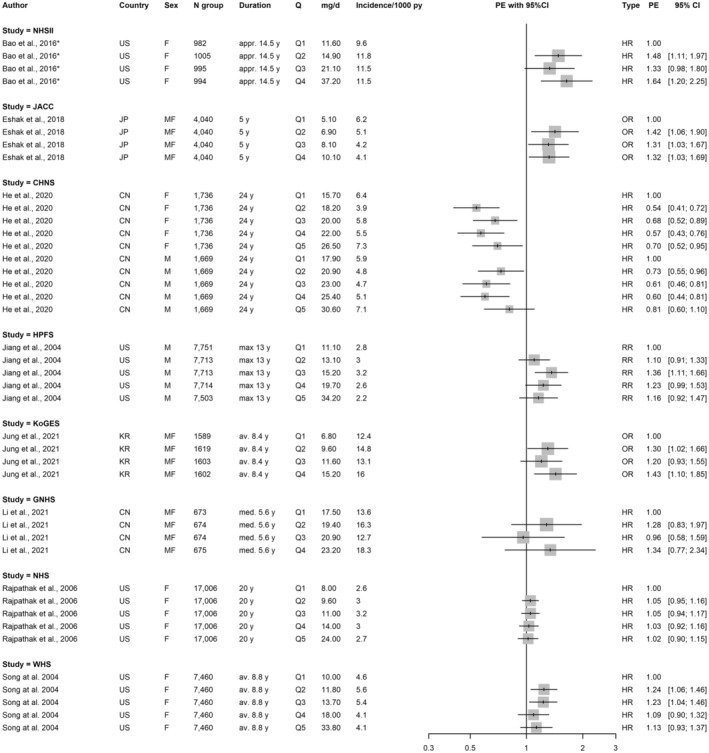
- Bao, W. , Chavarro, J. E. , Tobias, D. K. , Bowers, K. , Li, S. , Hu, F. B. , & Zhang, C. (2016). Long‐term risk of type 2 diabetes in relation to habitual iron intake in women with a history of gestational diabetes: A prospective cohort study. American Journal of Clinical Nutrition, 103, 375–381. 10.3945/ajcn.115.108712 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources