

The categorization of opaque pathologies outside of contrast media in hysterosalpingography which facilitate interpretation: A pictorial review
- PMID: 38868446
- PMCID: PMC11165221
- DOI: 10.18502/ijrm.v22i3.16163
The categorization of opaque pathologies outside of contrast media in hysterosalpingography which facilitate interpretation: A pictorial review
Abstract
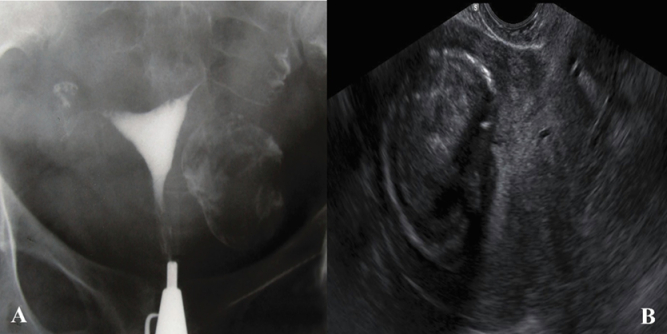
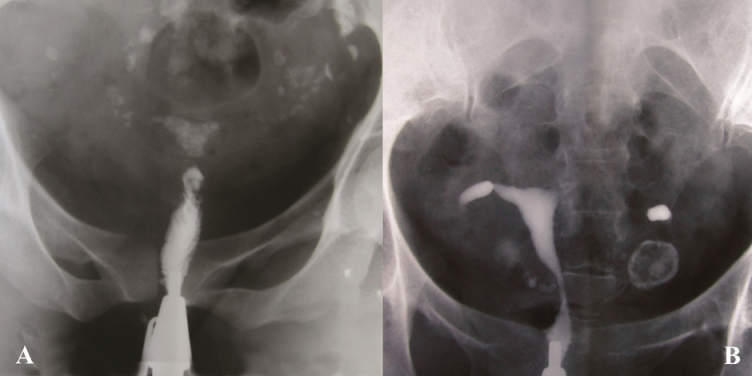
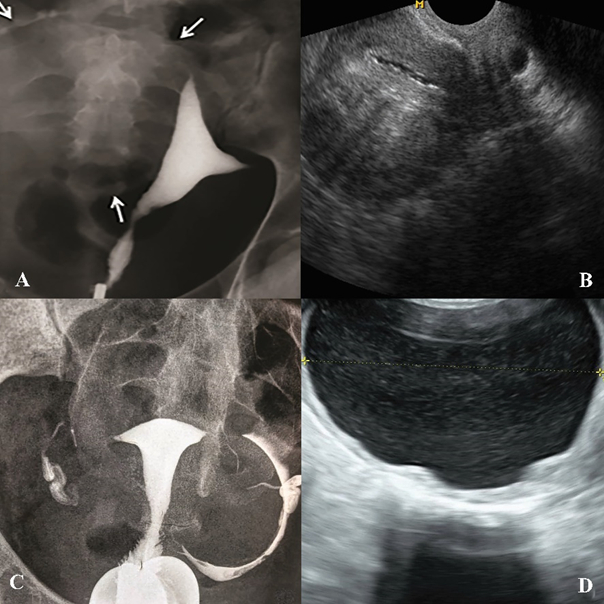
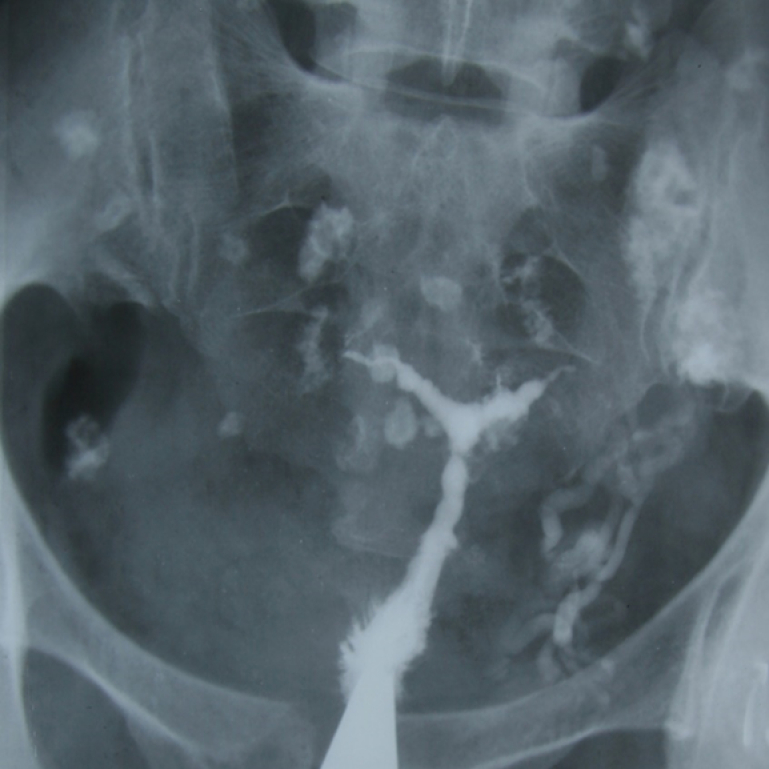
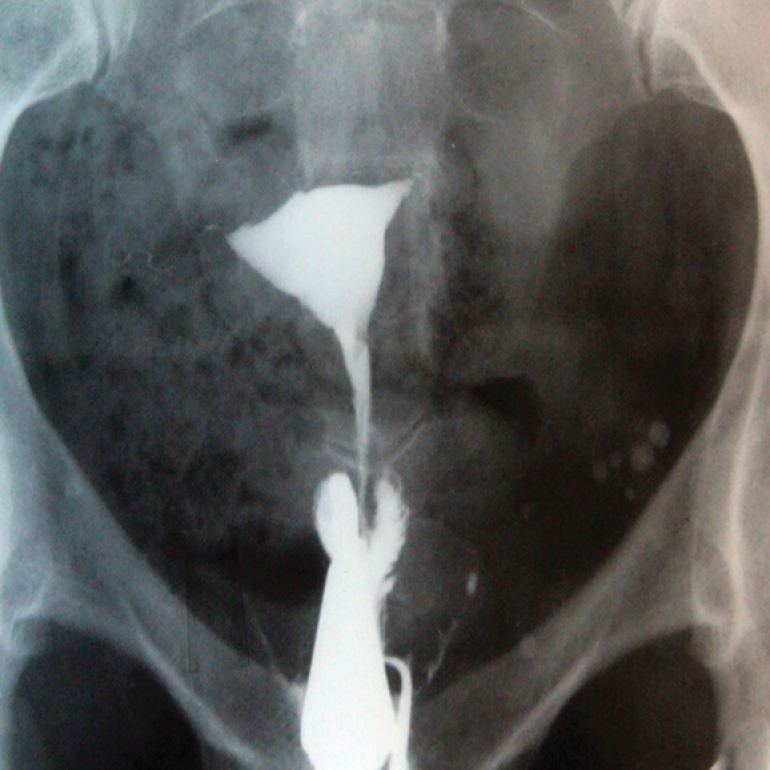
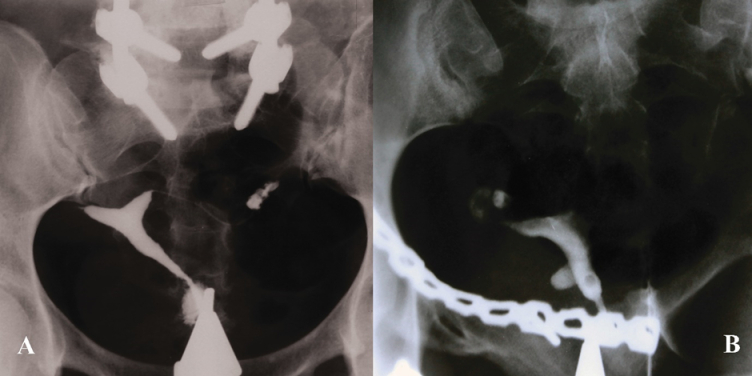
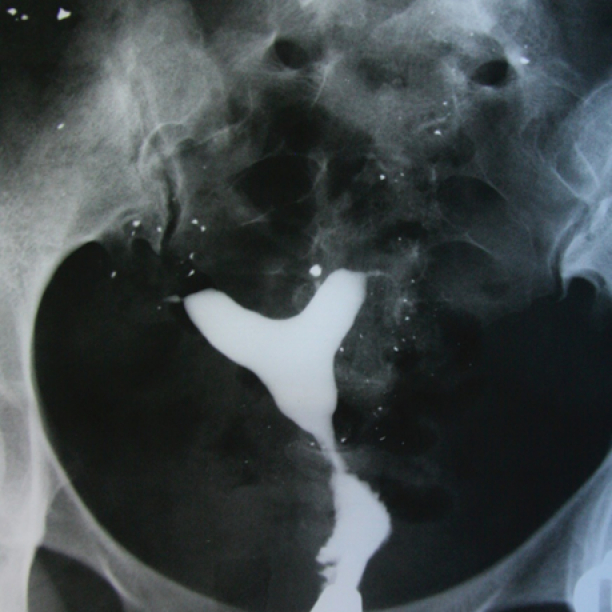
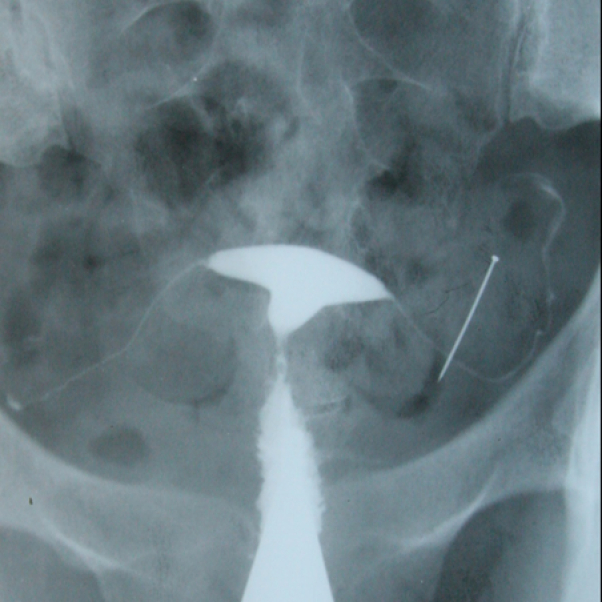
Hysterosalpingography (HSG) is a practical and reliable imaging method to evaluate the cervical canal, uterine isthmus, uterine cavity, and fallopian tubes. Using HSG, opaque pathologies outside of contrast media can be detected as well as pathologies of uterus and fallopian tubes. We aim to present and categorize some uncommon and interesting abnormal findings that are located outside of the contrast areas in HSG. This is a pictorial review that depicts various types of HSG images that include opaque pathologies outside of the contrast areas. Images have been extracted from valuable archives collected over 50 yr by professor Shahrzad. A plain pelvic film contains soft tissues of the pelvis, bony structures, artifacts, or foreign bodies. Categorization might easily help the radiologist to interpret the HSG cliché. Opaque pathologies outside of contrast area in HSG can be categorized into 2 groups: "Pelvic Tissue Related" and "Foreign Bodies". Pelvic tissue abnormalities might have a gynecologic or non-gynecologic source. Foreign bodies can be located in the pelvis or outside of the body. HSG is a reliable and inexpensive procedure. Familiarity with the pathologies of pelvic tissues and the accurate interpretation of HSG images are important.
Keywords: Abnormalities; Fallopian tubes.; Uterine; Hysterosalpingography; Opaque.
Copyright © 2024 Hosseini et al.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures








References
Publication types
LinkOut - more resources
Full Text Sources