

Diagnostic accuracy of endoscopic ultrasonographic shear wave elastography for assessing early chronic pancreatitis using the Japanese diagnostic criteria 2019
- PMID: 38868706
- PMCID: PMC11167156
- DOI: 10.1002/deo2.387
Diagnostic accuracy of endoscopic ultrasonographic shear wave elastography for assessing early chronic pancreatitis using the Japanese diagnostic criteria 2019
Abstract
Background and aim: Endoscopic ultrasound shear wave elastography (EUS-SWE) can facilitate an objective evaluation of pancreatic fibrosis. Although it is primarily applied in evaluating chronic pancreatitis, its efficacy in assessing early chronic pancreatitis (ECP) remains underinvestigated. This study evaluated the diagnostic accuracy of EUS-SWE for assessing ECP diagnosed using the Japanese diagnostic criteria 2019.
Methods: In total, 657 patients underwent EUS-SWE. Propensity score matching was used, and the participants were classified into the ECP and normal groups. ECP was diagnosed using the Japanese diagnostic criteria 2019. Pancreatic stiffness was assessed based on velocity (Vs) on EUS-SWE, and the optimal Vs cutoff value for ECP diagnosis was determined. A practical shear wave Vs value of ≥50% was considered significant.
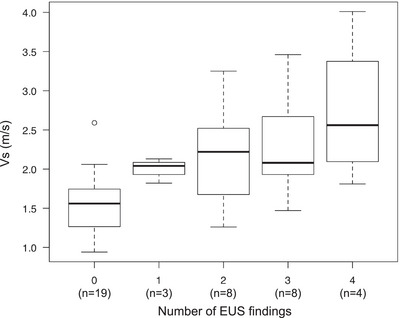
Results: Each group included 22 patients. The ECP group had higher pancreatic stiffness than the normal group (2.31 ± 0.67 m/s vs. 1.59 ± 0.40 m/s, p < 0.001). The Vs cutoff value for the diagnostic accuracy of ECP, as determined using the receiver operating characteristic curve, was 2.24m/s, with an area under the curve of 0.82 (95% confidence interval: 0.69-0.94). A high Vs was strongly correlated with the number of EUS findings (rs = 0.626, p < 0.001). Multiple regression analysis revealed that a history of acute pancreatitis and ≥2 EUS findings were independent predictors of a high Vs.
Conclusions: There is a strong correlation between EUS-SWE findings and the Japanese diagnostic criteria 2019 for ECP. Hence, EUS-SWE can be an objective and invaluable diagnostic tool for ECP diagnosis.
Keywords: acute pancreatitis; pancreatic fibrosis; propensity score; regression analysis; shear wave elastography.
© 2024 The Authors. DEN Open published by John Wiley & Sons Australia, Ltd on behalf of Japan Gastroenterological Endoscopy Society.
Conflict of interest statement
None.
Figures




References
-
- Witt H, Apte MV, Keim V, Wilson JS. Chronic pancreatitis: Challenges and advances in pathogenesis, genetics, diagnosis, and therapy. Gastroenterology 2007; 132: 1557–1573. - PubMed
-
- Braganza JM, Lee SH, McCloy RF, McMahon MJ. Chronic pancreatitis. Lancet North Am Ed 2011; 377: 1184–1197. - PubMed
-
- Singh VK, Yadav D, Garg PK. Diagnosis and management of chronic pancreatitis: A review. JAMA 2019; 322: 2422–2434. - PubMed
-
- Whitcomb DC, Shimosegawa T, Chari ST et al. International consensus statements on early chronic Pancreatitis. Recommendations from the working group for the international consensus guidelines for chronic pancreatitis in collaboration with The International Association of Pancreatology, American Pancreatic Association, Japan Pancreas Society, PancreasFest Working Group and European Pancreatic Club. Pancreatology 2018; 18: 516–527. - PMC - PubMed
LinkOut - more resources
Full Text Sources