

Liraglutide, a glucagon-like peptide-1 receptor agonist, inhibits bone loss in an animal model of osteoporosis with or without diabetes
- PMID: 38868747
- PMCID: PMC11167098
- DOI: 10.3389/fendo.2024.1378291
Liraglutide, a glucagon-like peptide-1 receptor agonist, inhibits bone loss in an animal model of osteoporosis with or without diabetes
Abstract
Introduction: Liraglutide (Lrg), a novel anti-diabetic drug that mimics the endogenous glucagon-like peptide-1 to potentiate insulin secretion, is observed to be capable of partially reversing osteopenia. The aim of the present study is to further investigate the efficacy and potential anti-osteoporosis mechanisms of Lrg for improving bone pathology, bone- related parameters under imageology, and serum bone metabolism indexes in an animal model of osteoporosis with or without diabetes.
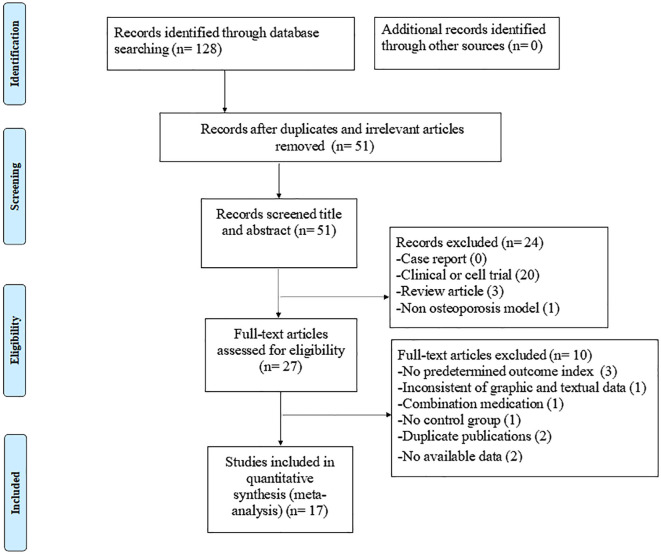
Methods: Eight databases were searched from their inception dates to April 27, 2024. The risk of bias and data on outcome measures were analyzed by the CAMARADES 10-item checklist and Rev-Man 5.3 software separately.
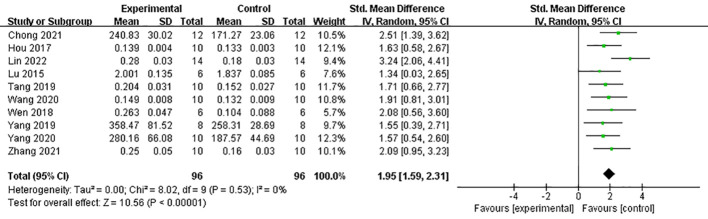
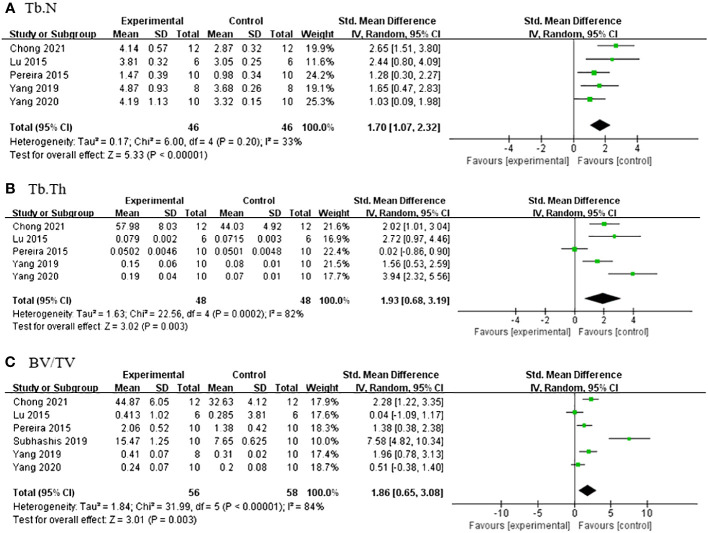
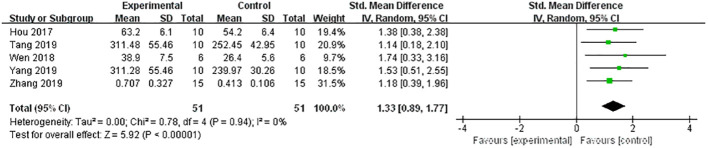
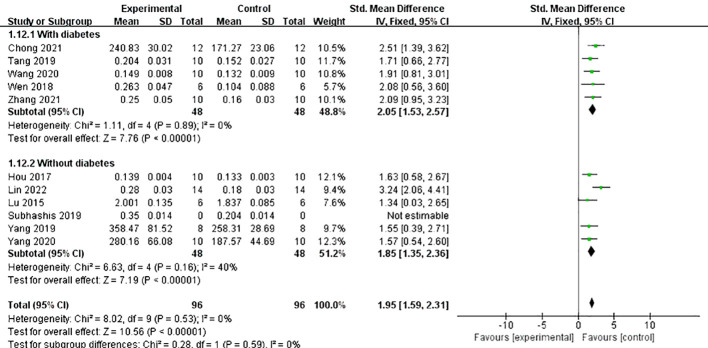
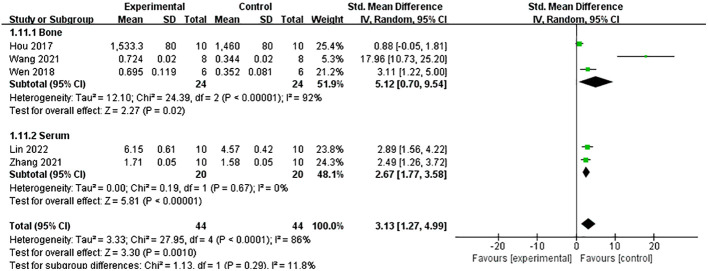
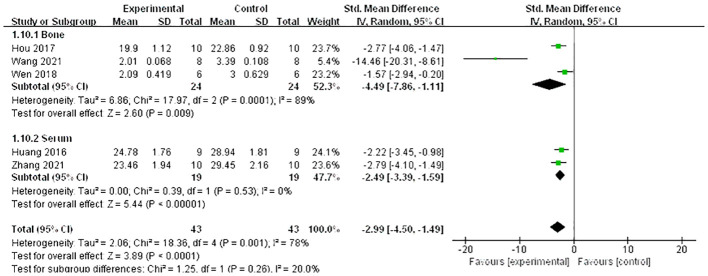
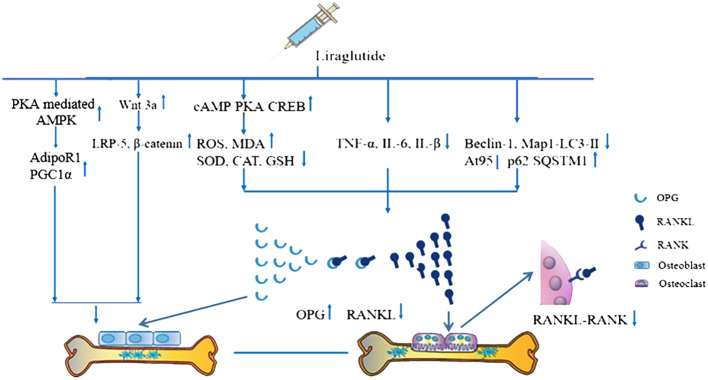
Results: Seventeen eligible studies were ultimately included in this review. The number of criteria met in each study varied from 4/10 to 8/10 with an average of 5.47. The aspects of blinded induction of the model, blinding assessment of outcome and sample size calculation need to be strengthened with emphasis. The pre-clinical evidence reveals that Lrg is capable of partially improving bone related parameters under imageology, bone pathology, and bone maximum load, increasing serum osteocalcin, N-terminal propeptide of type I procollagen, and reducing serum c-terminal cross-linked telopeptide of type I collagen (P<0.05). Lrg reverses osteopenia likely by activating osteoblast proliferation through promoting the Wnt signal pathway, p-AMPK/PGC1α signal pathway, and inhibiting the activation of osteoclasts by inhibiting the OPG/RANKL/RANK signal pathway through anti-inflammatory, antioxidant and anti-autophagic pathways. Furthermore, the present study recommends that more reasonable usage methods of streptozotocin, including dosage and injection methods, as well as other types of osteoporosis models, be attempted in future studies.
Discussion: Based on the results, this finding may help to improve the priority of Lrg in the treatment of diabetes patients with osteoporosis.
Keywords: diabetes; efficacy; liraglutide; osteoporosis; possible mechanisms.
Copyright © 2024 Wu, Deng, Ye, Xu, Han, Zheng and Zheng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Dipeptidyl-peptidase (DPP)-4 inhibitors and glucagon-like peptide (GLP)-1 analogues for prevention or delay of type 2 diabetes mellitus and its associated complications in people at increased risk for the development of type 2 diabetes mellitus.Cochrane Database Syst Rev. 2017 May 10;5(5):CD012204. doi: 10.1002/14651858.CD012204.pub2. Cochrane Database Syst Rev. 2017. PMID: 28489279 Free PMC article.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.Health Technol Assess. 2001;5(28):1-110. doi: 10.3310/hta5280. Health Technol Assess. 2001. PMID: 11701100
-
Gonadotropin-releasing hormone (GnRH) analogues for premenstrual syndrome (PMS).Cochrane Database Syst Rev. 2025 Jun 10;6(6):CD011330. doi: 10.1002/14651858.CD011330.pub2. Cochrane Database Syst Rev. 2025. PMID: 40492482 Review.
-
Insulin and glucose-lowering agents for treating people with diabetes and chronic kidney disease.Cochrane Database Syst Rev. 2018 Sep 24;9(9):CD011798. doi: 10.1002/14651858.CD011798.pub2. Cochrane Database Syst Rev. 2018. PMID: 30246878 Free PMC article.
-
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) for the treatment of type 2 diabetes mellitus: friends or foes to bone health? a narrative review of clinical studies.Endocrine. 2025 Jul;89(1):30-38. doi: 10.1007/s12020-025-04253-4. Epub 2025 May 8. Endocrine. 2025. PMID: 40342008 Free PMC article. Review.
Cited by
-
Glucagon-like peptide-1 receptor agonists: Exploring the mechanisms from glycemic control to treatment of multisystemic diseases.World J Gastroenterol. 2024 Sep 28;30(36):4036-4043. doi: 10.3748/wjg.v30.i36.4036. World J Gastroenterol. 2024. PMID: 39351253 Free PMC article.
-
Exploring new therapeutic drugs for osteoarthritis and osteoporosis: Glucagon-like peptide-1 receptor agonists: A review.Medicine (Baltimore). 2025 Jul 18;104(29):e43239. doi: 10.1097/MD.0000000000043239. Medicine (Baltimore). 2025. PMID: 40696619 Free PMC article. Review.
-
Use of GLP-1 receptor agonist and risk of osteoporosis among patients with type 2 diabetes: a real-world study.Front Endocrinol (Lausanne). 2025 May 21;16:1586589. doi: 10.3389/fendo.2025.1586589. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40469447 Free PMC article.
-
Glucose-Dependent Insulinotropic Polypeptide in Incretin Physiology: Role in Health and Disease.Endocr Rev. 2025 Jul 15;46(4):479-500. doi: 10.1210/endrev/bnaf006. Endocr Rev. 2025. PMID: 39951489 Free PMC article. Review.
-
Semaglutide promotes the proliferation and osteogenic differentiation of bone-derived mesenchymal stem cells through activation of the Wnt/LRP5/β-catenin signaling pathway.Front Pharmacol. 2025 Mar 10;16:1539411. doi: 10.3389/fphar.2025.1539411. eCollection 2025. Front Pharmacol. 2025. PMID: 40129942 Free PMC article.
References
-
- Chinese Association of Rheumatology and Immunology Physicians. Chinese Rheumatology Association. Chinese Society of Bone and Mineral Research. National Clinical Research Center for Dermatologic and Immunologic Diseases . Chinese consensus on the prevention and treatment of glucocorticoid induced osteoporosis. Zhong Hua Nei Ke Za Zhi. (2021) 60:13–21. doi: 10.3760/cma.j.cn112138-20201102-00914 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous